
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 36(1); 2011 > Article
- Case Report Management of white spots: resin infiltration technique and microabrasion
- Jeong-Hye Son, DDS, MS, Bock Hur, DDS, PhD, Hyeon-Cheol Kim, DDS, PhD, Jeong-Kil Park, DDS, PhD
-
2011;36(1):-71.
DOI: https://doi.org/10.5395/JKACD.2011.36.1.66
Published online: January 31, 2011
Department of Conservative Dentistry, Pusan National University School of Dentistry, Yangsan, Korea.
- Correspondence to Jeong-Kil Park, DDS, PhD. Associate Professor, Department of Conservative Dentistry, Pusan National University School of Dentistry, Beomeo-ri, Mulgem, Yangsan, Korea 626-770. TEL, +82-55-360-5213; FAX, +82-55-360-5214; jeongkil@pusan.ac.kr
• Received: November 2, 2010 • Revised: November 23, 2010 • Accepted: November 25, 2010
Copyright © 2011 Korean Academy of Conservative Dentistry
- 5,892 Views
- 50 Download
- 25 Crossref




Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Clinical Effectiveness of Resin Infiltration and Fluoride Varnish for Managing White Spot Lesions (International Caries Detection and Assessment System (ICDAS) ≤ 2) During Multibracket Orthodontic Treatment: A Systematic Review and Meta-Analysis
Vilius Kosys, Gabija Streimikyte, Giedre Trakiniene
Cureus.2026;[Epub] CrossRef - Resin Infiltration for the Esthetic Improvement of Dental Fluorosis and White Spots: A Case Report
Sumayyah L Alkhudhayri, Shahad L Alhassani, Nada A AbdelAleem
Cureus.2024;[Epub] CrossRef - White spot lesions in fixed orthodontic treatment: Etiology, pathophysiology, diagnosis, treatment, and future research perspectives
Suma Shankarappa, Jerusha Titus Burk, Pradeep Subbaiah, Raghunath Nagasundara Rao, Vidya Gowdappa Doddawad
Journal of Orthodontic Science.2024;[Epub] CrossRef - White Spot Lesions in Fixed Orthodontics: A Literature Review on Etiology, Prevention, and Treatment
Deem Al-Blaihed, Omar El Meligy, Khlood Baghlaf, Rabab A Aljawi, Shahad Abudawood
Cureus.2024;[Epub] CrossRef - Effectiveness of low-viscosity resin infiltration (Icon) on color change of enamel white spot lesions: 1-year follow-up clinical study
Mohamed. H. Zaazou, Reham S. Saleh, Shahinaz N. Hassan, Ali Abdelnabi, Zeinab M. Zaki, Tamer M. Hamdy, Dalia Y. Zaki, Lamiaa M. Moharam
Bulletin of the National Research Centre.2024;[Epub] CrossRef - Individual tooth segmentation in human teeth images using pseudo edge-region obtained by deep neural networks
Seongeun Kim, Chang-Ock Lee
Signal Processing: Image Communication.2024; 120: 117076. CrossRef - Surface topography and spectrophotometric assessment of white spot lesions restored with nano-hydroxyapatite-containing universal adhesive resin: an in-vitro study
Neven S. Aref, Rahaf M. Alsdrani
BMC Oral Health.2023;[Epub] CrossRef - Infiltrating Resins, Noninvasive Treatment of White Spot Lesions: A Case Report
Rubén Darío Miranda-Carreño, Jacqueline Adelina Rodríguez-Chávez, Abigailt Flores-Ledesma
Journal of Oral Health and Community Dentistry.2023; 17(2): 75. CrossRef - Management of Turner's Hypoplasia Using Resin Infiltration: A Case Report
Dhruvi Solanki, Punit Fulzele, Nilima Thosar, Unnati Shirbhate
Cureus.2023;[Epub] CrossRef - Colour Parameters and Changes of Tea-Stained Resin Composite Exposed to Whitening Pen (In Vitro Study)
Abdulaziz Alhotan, Rasha M. Abdelraouf, Saleh Alhijji, Merry Angelyn Tan De Vera, Aref Sufyan, Jukka P. Matinlinna, Tamer M. Hamdy
Polymers.2023; 15(14): 3068. CrossRef - Effect of Resin Infiltration and Microabrasion on the Microhardness of the Artificial White Spot Lesions (An in Vitro Study)
Reem Majeed H.J. Al-Mamoori, Aseel Haidar M.J. Al Haidar
Journal of Baghdad College of Dentistry.2022; 34(1): 44. CrossRef - Effect of sodium fluoride plus tricalcium phosphate with and without CO2 laser on remineralization of white spot lesions
Nouran M. Eissa, Eman M. Elshourbagy, Nahla E. Gomaa
Heliyon.2022; 8(10): e10752. CrossRef - Efficacy of Resin Infiltration and Fluoride Casein Phosphopeptide Amorphous Calcium Phosphate Varnish on Non-cavitated Active White Spot Lesions in Children: A Randomized Clinical Trial
Mohit Dhamija, Rish Tyagi, Namita Kalra, Amit Khatri
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2022;[Epub] CrossRef - Individual Tooth Segmentation in Human Teeth Images Using Pseudo Edge-Region Obtained by Deep Neural Networks
Seongeun Kim, Chang-Ock Lee
SSRN Electronic Journal .2022;[Epub] CrossRef - In Vitro, Influence Of In-Office Dental Whitening On The Color Of Teeth Treated With Resin Infiltration
Basil Almutairi, Mohammed Al-Refai, Bander AL-Meshary, Abdulrahman Al-Asim, Fahad Al-Sharidah, Abdullah Alshehri
Annals of Dental Specialty.2021; 9(4): 6. CrossRef - Evaluation of color changes of white spot lesions treated with three different treatment approaches: an in-vitro study
Shaza M. Hammad, Noha A. El-Wassefy, Mohamed A. Alsayed
Dental Press Journal of Orthodontics.2020; 25(1): 26. CrossRef - Spectrophotometric Evaluation of Color Change in Tooth Enamel Defects Using Resin Infiltrate: An In Vivo Study
Anil Gupta, Shikha Dogra, Sakshi Joshi, Vimanyu Kataria, Jyotika Saini, Monika Nagpal, Payal Narula
International Journal of Clinical Pediatric Dentistry.2020; 13(2): 150. CrossRef - Erosion Infiltration in the Management of Molar‐Incisor Hypomineralization (MIH) Defects
Rym Mabrouk, Souha Yahia, Afef Oueslati, Nadia Frih, Yuk Kwan Chen
Case Reports in Dentistry.2020;[Epub] CrossRef - Pediatric Dentists’ Educational Experiences, Attitudes, and Professional Behavior Concerning Resin Infiltration: Implications for Dental Education
Michael Jordan Halcomb, Marita R. Inglehart, Elisabeta Karl
Journal of Dental Education.2020; 84(3): 290. CrossRef - Esthetic improvements of postorthodontic white-spot lesions treated with resin infiltration and microabrasion: A split-mouth, randomized clinical trial
Xi Gu, Lin Yang, Deqin Yang, Yuan Gao, Xiaolei Duan, Xin Zhu, He Yuan, Jiyao Li
The Angle Orthodontist.2019; 89(3): 372. CrossRef - Effect of resin infiltration on the color and microhardness of bleached white‐spot lesions in bovine enamel (an in vitro study)
Sidika Aynur Horuztepe, Meserret Baseren
Journal of Esthetic and Restorative Dentistry.2017; 29(5): 378. CrossRef - Effect of Resin Infiltration on Artificial Caries: Anin vitroEvaluation of Resin Penetration and Microhardness
Deepesh Prajapati, Rashmi Nayak, Deepika Pai, Nagraj Upadhya, Vipin K Bhaskar, Pujan Kamath
International Journal of Clinical Pediatric Dentistry.2017; 10(3): 250. CrossRef - Application of quantitative light-induced fluorescence to determine the depth of demineralization of dental fluorosis in enamel microabrasion: a case report
Tae-Young Park, Han-Sol Choi, Hee-Won Ku, Hyun-Su Kim, Yoo-Jin Lee, Jeong-Bum Min
Restorative Dentistry & Endodontics.2016; 41(3): 225. CrossRef - Non-destructive management of white spot lesions by using tooth jewelry
Hee-Jin Kim, Lorena Karanxha, Su-Jung Park
Restorative Dentistry & Endodontics.2012; 37(4): 236. CrossRef - Color and hardness changes in artificial white spot lesions after resin infiltration
Ji-Hoon Kim, Ho-Hyun Son, Juhea Chang
Restorative Dentistry & Endodontics.2012; 37(2): 90. CrossRef
 ePub Link
ePub Link Cite
CiteManagement of white spots: resin infiltration technique and microabrasion

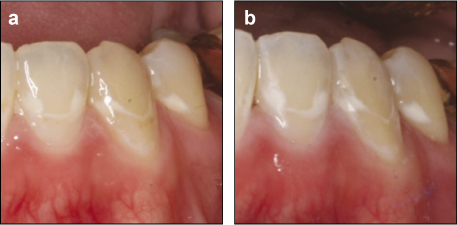
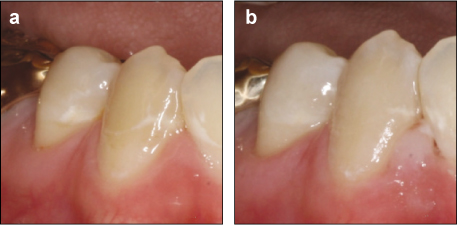
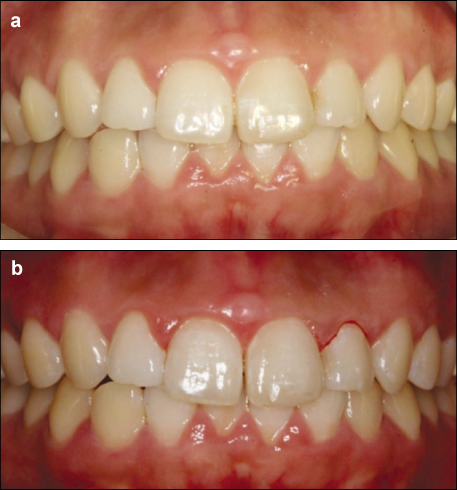
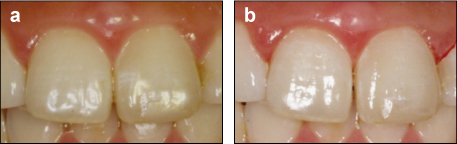
Figure 1
Intraoral photographs taken prior to treatment (a), after completion of resin infiltration technique (right side) and microabrasion (left side) (b).
Figure 2
Photographs of left mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of microabrasion (b).
Figure 3
Photographs of right mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of resin infiltration technique (b).
Figure 4
Intraoral photographs taken prior to treatment (a) and after completion of resin infiltration technique (left maxillary central incisor), microabrasion (right maxillary central incisor) and resin composite restoration (right maxillary lateral incisor) (b).
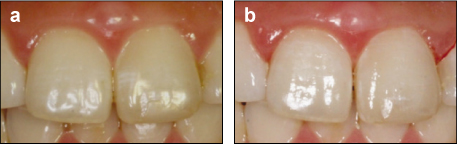
Figure 5
Photographs of maxillary central incisors taken prior to treatment (a) and completion of resin infiltration technique and microabrasion (b).
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Management of white spots: resin infiltration technique and microabrasion
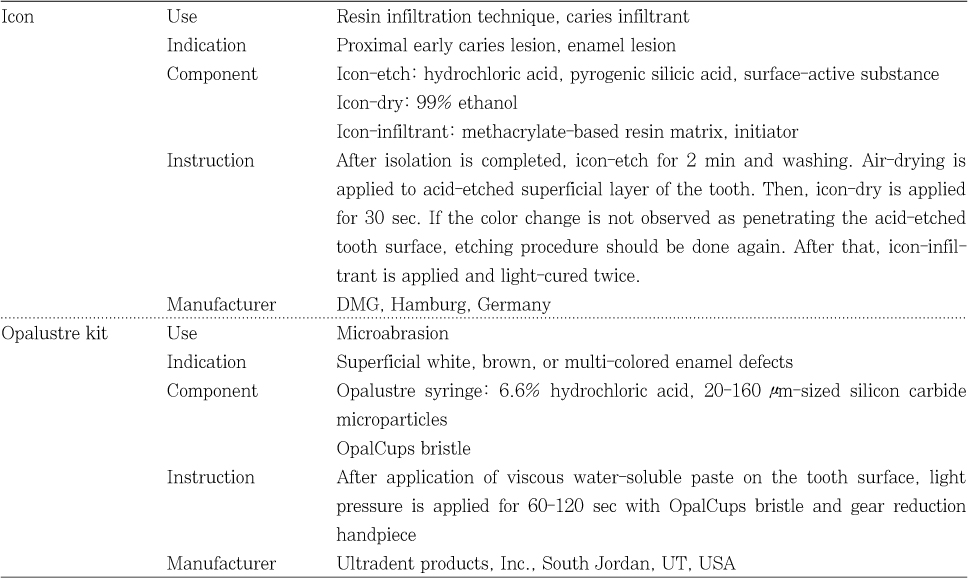
Materials used
Table 1
Materials used

