
Articles
- Page Path
- HOME > Restor Dent Endod > Ahead-of print articles > Article
- Review Article Educational implications of a novel system for classifying root and canal anatomy in the human dentition: a narrative review
-
Hany Mohamed Aly Ahmed1,*
 , Paul Michael Howell Dummer2
, Paul Michael Howell Dummer2 -
Restor Dent Endod [Epub ahead of print]
DOI: https://doi.org/10.5395/rde.2026.51.e28
Published online: May 20, 2026
1Department of Restorative Dentistry, Faculty of Dentistry, Universiti Malaya, Kuala Lumpur, Malaysia
2School of Dentistry, College of Biomedical and Life Sciences, Cardiff University, Cardiff, United Kingdom
- *Correspondence to Hany Mohamed Aly Ahmed, PhD Department of Restorative Dentistry, Faculty of Dentistry, Universiti Malaya, Jalan Universiti, Kuala Lumpur 50603, Malaysia Email: hany_endodontist@hotmail.com
• Received: September 15, 2025 • Revised: January 21, 2026 • Accepted: February 2, 2026
© 2026 The Korean Academy of Conservative Dentistry
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 876 Views
- 39 Download
- Abstract
- INTRODUCTION
- WHY WAS A NEW SYSTEM FOR CLASSIFYING TOOTH ANATOMY NEEDED?
- INTRODUCTION TO THE NOVEL SYSTEM FOR ROOT AND CANAL MORPHOLOGY
- INVOLVEMENT OF COMPLEMENTARY CODES FOR ACCESSORY CANALS
- COMPLEMENTARY CODES FOR DENTAL ANOMALIES
- APPLICATIONS OF THE AHMED CODING SYSTEM IN DENTAL EDUCATION
- DIRECTIONS FOR FUTURE RESEARCH
- CONCLUSIONS
- REFERENCES
Abstract
- A comprehensive understanding of both the external and internal anatomy of teeth is fundamental for the effective diagnosis and management of pulp and periapical pathoses. Recent progress in noninvasive, high-resolution imaging modalities, including cone-beam computed tomography and micro-computed tomography, has significantly enhanced the ability to examine the complex morphology of dental structures. These technological advancements have facilitated a level of anatomical detail that was previously unattainable, particularly in the assessment of crown, root, and canal systems. In response to this wealth of new anatomical data, a novel classification framework has been developed, enabling the systematic coding of root and canal configurations across all tooth types. This system offers a more nuanced and comprehensive representation of root canal anatomy compared to earlier classification models. This narrative review explores the implementation of this contemporary classification scheme in education, with a particular focus on its utility in recognizing anatomical variations and accessory canals for the benefit of undergraduate and postgraduate dental students as well as general dental practitioners.
INTRODUCTION
A comprehensive knowledge of root and canal morphology in the human dentition is essential for the success of endodontic therapies [1]. Over time, a variety of diagnostic modalities, including staining and clearing techniques, two-dimensional (2D) radiographic imaging, scanning electron microscopy, cone-beam computed tomography (CBCT), and micro-computed tomography (micro-CT), have been utilized in both research and clinical contexts to investigate dental anatomy [2–7]. It is widely recognized that considerable variation exists in root and canal configuration, depending on the type of tooth and the population studied [1,7].
The purpose of classification within scientific disciplines is to systematically organize knowledge and to delineate the defining features of the entities being classified [8]. From the pioneering investigations by Hess and Zürcher [2] to contemporary research, there has been a growing recognition of the need for a comprehensive system to describe root and canal morphology across all tooth types and anatomical variations. The Vertucci classification [3] has historically been the most commonly adopted framework for categorizing canal configurations. However, its limitations have been increasingly highlighted in recent studies, which demonstrate that the system does not adequately accommodate the full spectrum of anatomical diversity encountered in clinical practice [9,10]. In light of this shortcoming, a new coding system has been introduced to standardize the classification of root and canal anatomy [9]. This contemporary approach has demonstrated accuracy in both laboratory-based and clinical observational studies [10]. The present article aims to summarize the structure and utility of this novel system, with particular emphasis on its implications for dental education.
WHY WAS A NEW SYSTEM FOR CLASSIFYING TOOTH ANATOMY NEEDED?
Using tooth sectioning and 2D radiographic techniques, Weine et al. [4,11] initially classified root canal configurations (RCCs) into four distinct types (Figure 1A). Vertucci et al. [12] subsequently described eight canal types (Figure 1B) with further reports [13–16] identifying 15 other canal configurations to complement Vertucci’s original classification [3] (Figure 1C). Later, a range of canal configurations that could not be classified within the existing systems were introduced [17].
The classification system introduced by Vertucci et al. [12], along with its supplementary categories, has been the most widely adopted and has proven useful in categorizing numerous canal configurations. However, there are significant limitations within the system, including:
The classification of Vertucci et al. [12] organizes RCCs into distinct types; however, it does not provide codes or descriptions for the number of roots or their specific location in anterior and premolar teeth. This limitation leads to several issues.
a) It is impossible to distinguish between a Vertucci type IV canal (which has two separate root canals) in a single-rooted or a double-rooted tooth (Figure 2 [18]), as the number of roots is not specified.
b) Vertucci type V canals (which can have one or two canals) may occur in either single-rooted or double-rooted teeth, but this distinction is not addressed in the system.
c) Maxillary (or mandibular) premolars (or anterior teeth) with three canals are classified as Vertucci type VIII, without accounting for the number of roots or the position of the canal bifurcations along the root.
This lack of detail reduces the accuracy and thus the utility of canal classifications in these specific tooth types.
The absence of this critical information on the number of roots has significant implications for the clinical management of teeth undergoing root canal treatment and endodontic surgery. One key area affected is access cavity preparation, where premolar teeth with varying root numbers typically have canal orifices located in different positions [19]. Additionally, root canal instrumentation and the preparation for intracanal posts differ in double-rooted maxillary premolars, particularly because of the reduced dentine thickness near the furcation groove on the palatal aspect of the buccal root [19] (Figure 3). In certain cases, the buccal root of double-rooted maxillary premolars may feature deep grooves on both the buccal and palatal surfaces (Figure 3C), further complicating treatment planning.
In addition to the number of roots, the location of the roots is also a crucial factor that the Vertucci system does not define. This lack of information can lead to difficulties in accurately classifying certain tooth configurations. Examples where root location is important include:
a) Anterior teeth with two roots can occur in two forms: either as mesial and distal or buccal and palatal/lingual roots [20].
b) Double-rooted mandibular premolars can present with two variations: either with mesial and distal root locations or with buccal and lingual root locations [10] (Figure 4).
c) Maxillary premolars with three roots can appear in a range of configurations, such as having two buccal roots and one palatal root or one buccal root and two palatal roots [19,21].
These variations in root location are important for treatment planning but are not adequately addressed by the Vertucci classification system.
The Vertucci classification lacks precise definitions for key root canal components, such as the canal orifice. In a subsequent publication, Vertucci [1] described the canal orifice as “a root canal begins as a funnel-shaped canal orifice generally present at or slightly apical to the cervical line.” However, this definition lacks clarity regarding what is meant by “slightly apical” to the cervical line. One possible reason for this ambiguity is that the Vertucci classification was based on decalcified, stained teeth, where the preparation process and immersion in strong acids can significantly degrade a tooth’s normal anatomical features, including the cementoenamel junction (CEJ). As a result, accurately identifying the CEJ on such specimens is challenging [22].
It is also important to note that, in multi-rooted teeth, the location of the pulp chamber floor may not align with the CEJ [1,23], further complicating the Vertucci system’s applicability in such cases.
An intercanal communication has been defined by the American Association of Endodontists [24] as “a thin communication between two or more canals in the same root or between vascular elements in tissues.” However, there is ongoing confusion and a lack of consensus regarding whether such a communication should be considered an integral part of the RCC, influencing its classification, or whether it should be regarded as a minor feature that does not affect the anatomical classification of the main canal system. This issue has been discussed in the literature, with differing views on its significance [25] (Figure 5).
Classifying root canals using the Vertucci classification becomes more complex when intercanal communications are considered as part of the main canal configuration (Figure 5). Since Vertucci [3] did not specify criteria for defining intercanal communications, this leads to further confusion, especially when micro-CT studies report many canal configurations as “Vertucci non-classifiable types” [26,27]. Several observational CBCT clinical studies either have not included transverse canals as part of the RCC or have failed to clarify the criteria for defining transverse canals when they are not meant to be considered [6,28,29]. This variation in interpretation has led to conflicts when comparing studies, not only due to the use of different diagnostic tools and study models, but also because the same classification system is being applied inconsistently [10].
Classifying a transverse canal anastomosis separately from the main RCC raises concerns due to its clinical significance during various stages of conventional root canal treatment. These stages include canal preparation, filling, as well as root-end cavity preparation and filling during surgery [30–32]. Additionally, a transverse canal anastomosis may communicate with the external root surface, potentially allowing microorganisms and their associated toxins to come into contact with the lateral periodontal and periapical tissues [33]. This highlights the importance of considering such anatomical features in diagnosis and treatment planning.
Defining RCCs using a simple scheme of Roman numerals as done with the Vertucci system has proven to be inadequate, as numerous studies have highlighted the complexity of root canal anatomy in human teeth with many canal configurations being identified as “Vertucci non-classifiable types” [27,34–36]. This underscores the impracticality of using a limited set of Roman numerals to accurately describe the wide variety of canal configurations, making it clear that a more comprehensive system is needed.
INTRODUCTION TO THE NOVEL SYSTEM FOR ROOT AND CANAL MORPHOLOGY
A novel coding system for classifying root and canal morphology was introduced by Ahmed et al. [9], offering comprehensive details on tooth notation, the number of roots, and RCCs. The purpose of this novel system was to establish an accurate and practical framework for use by undergraduate and postgraduate students, clinicians, and researchers. It enables the classification of root and canal configurations when using various methods of tooth examination, ensuring greater consistency and clarity in the assessment of tooth anatomy.
The Ahmed et al.’s classification system [9] comprises codes for three distinct components: tooth number (TN), number of roots, and RCC (Figures 6, 7).
The TN can be expressed using any standard numbering system. In cases where a tooth cannot be identified using one of these systems (e.g., extracted teeth of unknown origin), an appropriate abbreviation may be used. For example, the upper (maxillary) central incisor may be abbreviated as UCI.
The number of roots (R) is indicated as a superscript before TN (RTN). For example, 1TN means that tooth ‘TN’ has one root; 2TN means that the tooth has two roots and so on.
The RCC for each root is indicated as a superscript number(s) following the TN. This defines the continuous course of the root canal system, starting from the root canal orifice (O), passing through the canal (C), and ending at the foramen (F) (or foramina). The system specifies that the root canal orifice begins at the CEJ in single-rooted teeth and at the level of bifurcation in multi-rooted teeth.
In certain cases, the root bifurcation in multi-rooted teeth occurs in the middle or apical third of the root. In these instances, a common canal may be present coronally, starting at the level of the CEJ, similar to single-rooted teeth. This common canal is indicated as a superscript before describing the canal configuration for each of the roots (Figure 7). Recently, the coding system has been further applied in the primary dentition [37].
INVOLVEMENT OF COMPLEMENTARY CODES FOR ACCESSORY CANALS
When necessary, the coding system can also be used to classify accessory canals in conjunction with main canal configurations within a single code. The root length is divided into three sections: coronal third (C), starting from an imaginary line at the most apical portion of the pulp chamber; middle third (M); and apical third (A). Each of these thirds is identified as a superscript within parentheses following the RCC. In some cases, an accessory canal may not terminate in a foramen. In such instances, the code (1‐0) indicates a blind accessory canal, and the code (2‐1‐0) denotes a looped accessory canal. Figure 8 illustrates the application of the new coding system for accessory canals.
COMPLEMENTARY CODES FOR DENTAL ANOMALIES
The coding system can be adapted to classify root anomalies and their subtypes. The abbreviation for each anomaly (A) can be added within brackets. For example, (DE) refers to “dens evaginatus” affecting a specific tooth (Figure 9).
• When a tooth has two or more different developmental anomalies, a comma (,) should be placed between the initials of each anomaly (A1, A2). For example, (DI, RD) refers to a tooth with both dens invaginatus (DI) and root dilaceration (RD).
• A slash (/) should be used to describe fused teeth, such as when one tooth is fused to a supernumerary tooth, or when roots are fused in double-rooted teeth. Two slashes (//) should be used to indicate fused teeth or roots with intercommunications in the root canals.
• The subtype of each anomaly (if applicable) should be written as a superscript following the anomaly abbreviation. For instance, (DII) refers to a tooth with dens invaginatus type II [38,39].
APPLICATIONS OF THE AHMED CODING SYSTEM IN DENTAL EDUCATION
Understanding the external and internal anatomical variations of tooth roots is essential for successful root canal treatment and a range of other endodontic therapies [40,41]. Dental anatomy plays a pivotal role in the endodontic curriculum and serves as the foundation for students to grasp the complexities of root canal systems before progressing to clinical practice. Survey studies are valid research tools that provide information on feedback and behaviors of respondents [42], and they enable continued assessment and evaluation of new trends in endodontic education [43].
To date, four survey studies compared the Ahmed coding system to the Vertucci system [44–47]. Three of these studies used a validated questionnaire [44–46], in which a Microsoft PowerPoint (PPT) presentation (35 slides; Microsoft Corp., Redmond, WA, USA) was prepared with three components: (i) introduction; (ii) Vertucci classification (and its supplemental configuration types); and (iii) Ahmed coding system together with examples of teeth interpreted using both systems. For consistency, the description of the two classification systems had the same number of slides, font size, slide background, and transition animations; however, since the new system comprises codes with superscripts, the font size of the codes to define root and canal morphology was made larger to allow better visibility. To ensure transparency, the presenters of the PPT presentations in the three studies were independent and did not contribute to the development of the Ahmed coding system.
The fourth study [47] examined the incorporation of small-group practical seminars into a traditional lecture format to improve the understanding of both systems in addition to the Weine classification. The three systems were supported by a brief PPT presentation showing schematic and radiographic images of different canal configurations. This was followed by a practical exercise that included a template showing the external anatomy of the different dental groups, in which the student was requested to draw several internal anatomies based on the different classifications. Table 1 shows the details of the four studies included in this review.
The first survey conducted among 382 undergraduate dental students from eight Malaysian dental schools revealed that over 90% of students reported that the Ahmed system was more accurate and practical compared to the Vertucci system and its supplemental configurations [44]. More than 95% of students reported that the new coding system improved their understanding of root canal morphology and that they would recommend its inclusion in both preclinical and clinical courses. The positive feedback observed among undergraduate students was similarly echoed by postgraduate dental students in the same study, emphasizing the system’s utility in advanced learning [44], similar to the second study done in Peru [45]. The large-scale study in India involving 1,082 participants from 13 dental schools reported that 93% of participants found the Ahmed classification system to be more practical and accurate compared to the Vertucci system [46].
Figure 10 summarizes the survey results from various studies that used the same questionnaire, comparing the responses from dental students, postgraduate students, and practitioners about the practicality and accuracy of the Ahmed coding system versus the Vertucci classification. The results indicate a clear preference for the Ahmed system, which supports its potential for widespread implementation in dental education worldwide.
In the fourth survey study [47], 98.8% of students agreed that the Ahmed classification system was the most complete, and 84% of students found it to be the most intuitive. However, 67% of students reported that the Ahmed system was the most difficult to understand. Despite this difficulty, all students believed that the small-group practical seminars helped them better understand the Ahmed coding system. This study demonstrates that, while the Ahmed system may initially seem complex, the use of interactive seminars significantly enhanced students’ comprehension and application of the system, reinforcing the concept that hands-on learning can be an effective tool for understanding complex dental anatomy.
The positive feedback regarding the Ahmed coding system can be attributed to several key factors.
1. Open system for comprehensive classification
The coding system is an “open system,” meaning it is flexible and adaptable. It is capable of accurately classifying the number of roots and their canal configurations for all teeth, whether simple or complex. This flexibility allows for a more comprehensive approach to classifying root canal systems, offering a greater level of detail than other systems that may be limited to specific types of canal configurations.
2. No memorization of Roman numerals
Unlike the Vertucci classification, which relies on Roman numerals for categorizing RCCs, the Ahmed system does not require users to memorize a set of predefined categories. This user-friendly approach simplifies the learning process, as it allows for a more intuitive and flexible method to describe RCCs without being constrained by a rigid classification system. This flexibility makes it easier for both students and clinicians to apply the system in practice.
3. Student reflections and expanding possibilities
The survey conducted among Malaysian dental students focused primarily on RCCs; however, students expressed interest in extending the system’s application to classify other anatomical features such as accessory canals and anomalies [44]. This feedback highlights the ability of students to think critically about how the system can be adapted to other areas of dental anatomy. Such reflections indicate that students are not only grasping the principles of the system but also developing a deeper understanding of the subject. They are able to apply, analyze, and extend their knowledge in line with Bloom’s taxonomy, which emphasizes the importance of learners creating and expanding on existing knowledge [48].
In conclusion, the Ahmed coding system is favored for its flexibility, simplicity, and ability to accurately describe complex anatomical features. Its “open system” structure makes it an effective educational tool that is applicable to the entire range of RCCs, accessory canals, and anomalies. Student feedback and the potential of the system for further expansion underscore its value in enhancing both dental education and clinical practice. This adaptability and the possibility of future improvements suggest that the system can evolve as new anatomical knowledge is acquired, making it a dynamic tool for understanding and classifying dental anatomy. The widespread positive feedback supports its integration into dental curricula across the globe, with students and practitioners recognizing its value in accurately diagnosing and classifying complex root canal systems. These findings, however, should not undermine the value of previous classification systems. Dental practitioners should remain aware of the advantages and limitations of each system. Despite its limitations, the Vertucci classification has been widely used for more than four decades. Its eight canal configuration types can describe many root canal configurations in the human dentition and facilitate comparison with previous studies.
While the Ahmed coding system has demonstrated significant advantages in classifying complex root canal anatomies and providing greater detail compared to other systems, it is important to recognize its limitations, which need to be considered by dental professionals, educators, and researchers when applying this classification in practice.
1. Increased number of groupings
One of the limitations of the Ahmed system is that it often results in a larger number of groupings for teeth with more intricate canal anatomical features, especially in cases involving multi-rooted teeth (maxillary and mandibular premolars and molars), examined using highly accurate devices such as micro-CT which allows the visualization of fine canal branchings and even the smallest accessory canals that may not be visible with other methods [10,49–52].
This increased number of groups has also been documented in previous CBCT studies [53–55]. A recent study [56] compared root and canal anatomy in maxillary first premolars in 22 countries using both the Ahmed and Vertucci systems and concluded that the Ahmed coding system was more accurate and comprehensive than the Vertucci system. However, a larger number of groups was observed when using the Ahmed system because it takes into account the number of roots (so each single, double, and three-rooted variant will have separate codes) in addition to the complex canal anatomy that was allocated with separate codes corresponding to the large number of non-classifiable Vertucci types.
This expanded number of tooth groups in micro-CT and CBCT anatomy studies might appear overwhelming to some users, particularly those unfamiliar with the finer details of tooth anatomy. While this increased granularity may seem complex, it allows for a more precise categorization of complex canal configurations, providing clinicians with specific and accurate information to plan treatments accordingly [10]. This is also important for accurate comparisons between research studies.
Traditional 2D radiographs can be helpful for basic canal classification, but often lack the detail required for identifying complex anatomical features or subtle canal variations. As a result, the classification of canal anatomy using 2D images leads to fewer groups but is less accurate than those obtained using more advanced three-dimensional (3D) imaging techniques [57].
2. Learning curve
Given the detailed nature of the Ahmed coding system, it requires a learning curve for dental students and practitioners who are new to this approach, especially when classifying multi-rooted teeth with common canals (Figure 8), and when the complementary codes are used to classify teeth with multiple roots, canal configurations, accessory canals, and anomalies [44]. As mentioned above, the use of interactive seminars enhances the comprehension and understanding of root canal anatomy classifications [47].
DIRECTIONS FOR FUTURE RESEARCH
The Ahmed coding system plays an essential role not only in classifying root canal anatomy but also in determining the difficulty level of a particular case scheduled for root canal treatment. This is particularly important in clinical practice, especially when the operator is an undergraduate dental student, a postgraduate student, or a general dental practitioner (GDP).
Taking into account the inherent limitations of diagnostic 2D periapical imaging, it is crucial that each case be appropriately assessed according to the operator’s level of knowledge and skill, so the level of complexity is tackled at the appropriate stage of their education or career. This would provide them with a structured approach to anticipate challenges and plan accordingly, and also ensure optimal patient care and minimize the risk of errors or complications during treatment. For example, a tooth code of 214 B1 P1 refers to a double-rooted maxillary molar tooth (tooth 14), where each root (B and P) has a single canal. This is a relatively straightforward case and most likely suitable for an undergraduate dental student or a GDP. A tooth code of (RE) 346 M2 D1 DL1 refers to a three-rooted mandibular molar tooth (tooth 46) (RE refers to radix entomolaris), where the mesial root (M) has two separate canals and each of the distal root (D) and disto-lingual root (DL) has a single canal. Given the usual buccal curvature of the DL root, the case would be more challenging for a dental student or GDP and would be more suitable for an endodontic specialist. Indeed, the availability of CBCT data would provide more detailed codes and thus a more accurate case difficulty assessment process.
Future studies should also assess the effectiveness of the system in improving students’ understanding of root and canal morphology and the consistency of students’ ability to apply the system, especially in identifying different canal configurations across various tooth types. The evaluation of the coding system by researchers in different countries with various educational backgrounds and teaching models is needed. The implementation of calibration sessions, particularly for undergraduate and postgraduate students, as well as for practitioners unfamiliar with the system, would be beneficial to ensure that the Ahmed coding system is applied consistently by different users. This would help ensure that the system is used in a uniform manner across different clinical and educational settings.
Several studies have explored innovative teaching methods to improve the understanding of root canal anatomy by dental students. Reymus et al. [58] reported favorable feedback from third-year undergraduate students who were taught root canal anatomy using virtual reality (VR). The VR application incorporated the Ahmed coding system for classifying the CBCT scanned teeth where the Digital Imaging and Communications in Medicine (DICOM) files were converted to Standard Tessellation Language (STL) files imported into a VR software and viewed in a head-mounted VR device. The VR environment helped students to interact with 3D models of teeth and visualize RCCs in a more engaging and dynamic way. The immersive experience of VR likely helped students grasp complex anatomical concepts more effectively.
Another study [59] utilized STL files from DICOM files of micro-CT scanned teeth classified using the Vertucci and Ahmed coding system; the researchers used a software application that was designed to be compatible with Android handheld devices for augmented reality and VR devices. By combining interactive digital technologies with traditional teaching methods, this approach allowed students to visualize and manipulate root canal systems in a highly interactive environment. The use of this technology further enhanced students’ understanding of root canal anatomy and the various classification systems. Future studies can use micro-CT scanned models for the development of a VR environment presenting the complementary codes of the Ahmed et al. system, thus integrating the main and accessory canals in a single code, as shown in Figure 11. This can also be applied to dental anomalies and the anatomical variations in the primary dentition.
A recent review discussed potential applications of artificial intelligence (AI) in root canal anatomy education [60]. The use of real-time AI-assisted analysis of 2D and CBCT imaging is a promising platform for root canal anatomy education of dental students and classifications of root and canal configurations using the novel coding system. Deep learning models that guide students to focus on certain landmarks on enhanced 2D radiographic images may help improve their skills and their ability during case difficulty assessment. The AI platform can also provide guidelines to help students navigate through the steps involved in the management (including access cavity preparation, instrumentation plan, and root canal filling) of different canal types, ranging from simple to more complex codes. However, it has to be acknowledged that the development of accurate AI models suitable for educational purposes requires large, diverse datasets for training and validation. Clinical exploration of canals remains an important step for the identification and classification of roots and canals. At present, AI applications should be used in root and canal anatomy education with caution, since they may generate incorrect recommendations if there is an over-reliance on technology based on limited patient data [61]. AI applications for the use of the Ahmed coding system in different imaging and education tools require further research.
CONCLUSIONS
The Ahmed coding system has shown considerable promise for classifying root and canal anatomy, particularly in teeth with multiple roots and/or complex canal anatomy. The integration of technology-enhanced educational approaches, such as 3D imaging and interactive learning platforms, significantly enhances comprehension of root and canal anatomy when interpreted using contemporary classification systems. However, dental students, educators, and clinicians must be aware of the strengths and limitations of these systems. Future research is needed to explore AI applications in improving the interpretation and classification of root and canal anatomy.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING/SUPPORT
The authors have no financial relationships relevant to this article to disclose.
-
AUTHOR CONTRIBUTIONS
Conceptualization, Methodology: Ahmed HMA, Dummer PMH. Writing - original draft: Ahmed HMA. Writing - review & editing: Ahmed HMA, Dummer PMH. All authors read and approved the final manuscript.
PMHD: Conceptualization, Methodology, Writing - review & editing.
-
DATA SHARING STATEMENT
The datasets are not publicly available but are available from the corresponding author upon reasonable request.
Figure 1.
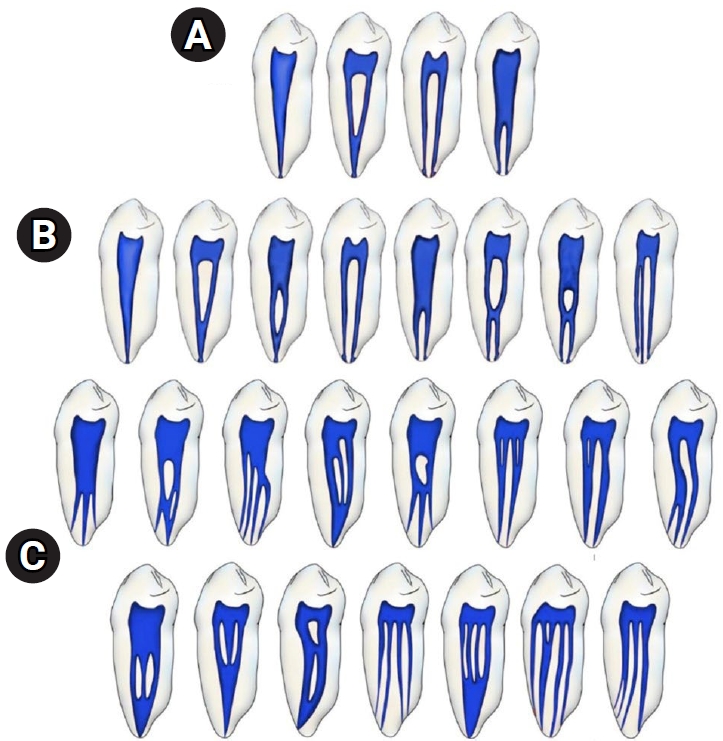
Common classifications of root canal configurations. (A) Weine et al.’s classification [11]: types I (1), II (2-1), III (2), and IV (1-2). (B) Vertucci et al.’s classification [12]: types I (1), II (2-1), III (1-2-1), IV (2), V (1-2), VI (2-1-2), VII (1-2-1-2), and VIII (3). (C) Supplemental configurations of the Vertucci classification [13–16]: types IX (1-3), X (1-2-3-2), XI (1-2-3-4), XII (2-3-1), XIII (1-2-1-3), XIV (4-2), XV (3-2), XVI (2-3), XVII (1-3-1), XVIII (3-1), XIX (2-1-2-1), XX (4), XXI (4-1), XXII (5-4), and XXIII (3-4).
Figure 2.
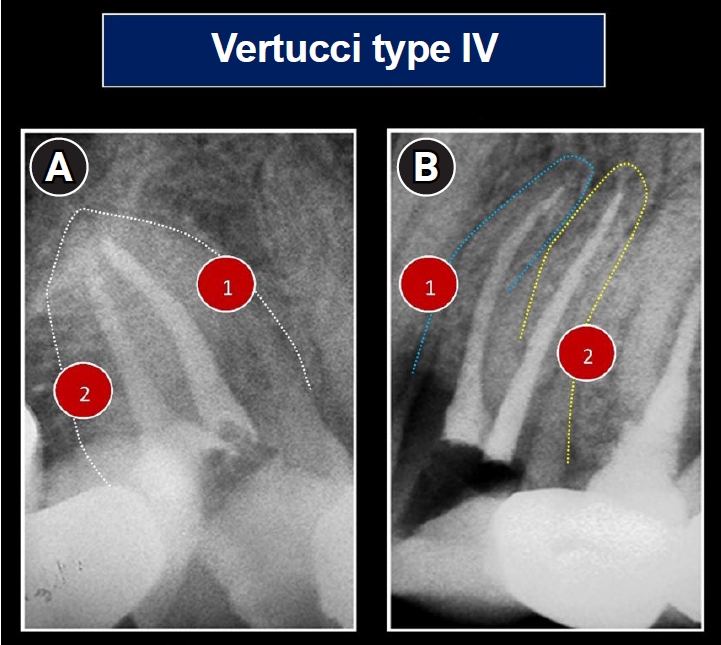
Periapical radiographs of a single-rooted (A) and double-rooted (B) maxillary premolar which are classified the same using the Vertucci classification, that is, type IV (two separate canals). Reproduced and modified from Ahmed et al. [18], according to the Creative Commons License.
Figure 3.
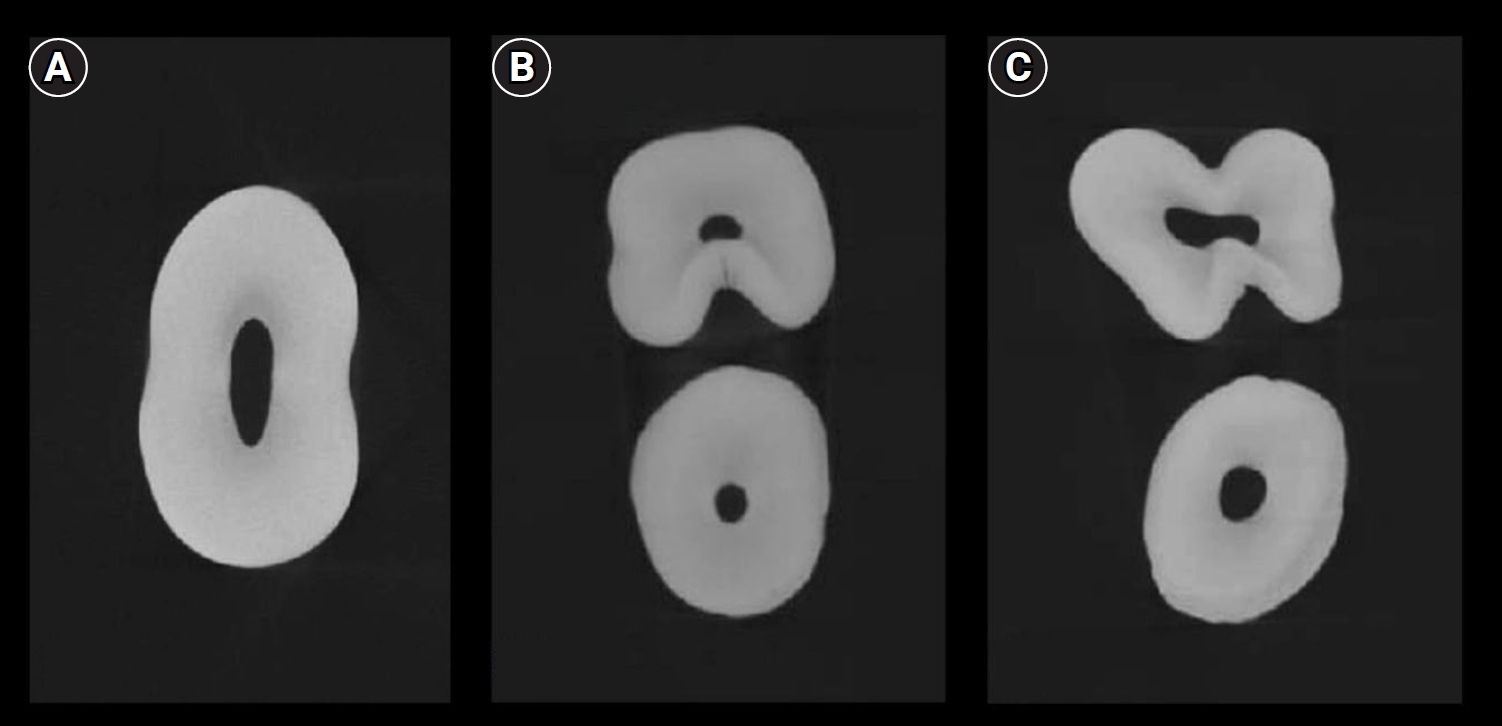
Micro-computed tomography images showing the morphological variations in the axial sections of maxillary premolars: (A) single-rooted; (B) double-rooted with a furcation groove in the palatal aspect of the buccal root; and (C) double-rooted with developmental grooves in the buccal and palatal aspects of the root.
Figure 4.
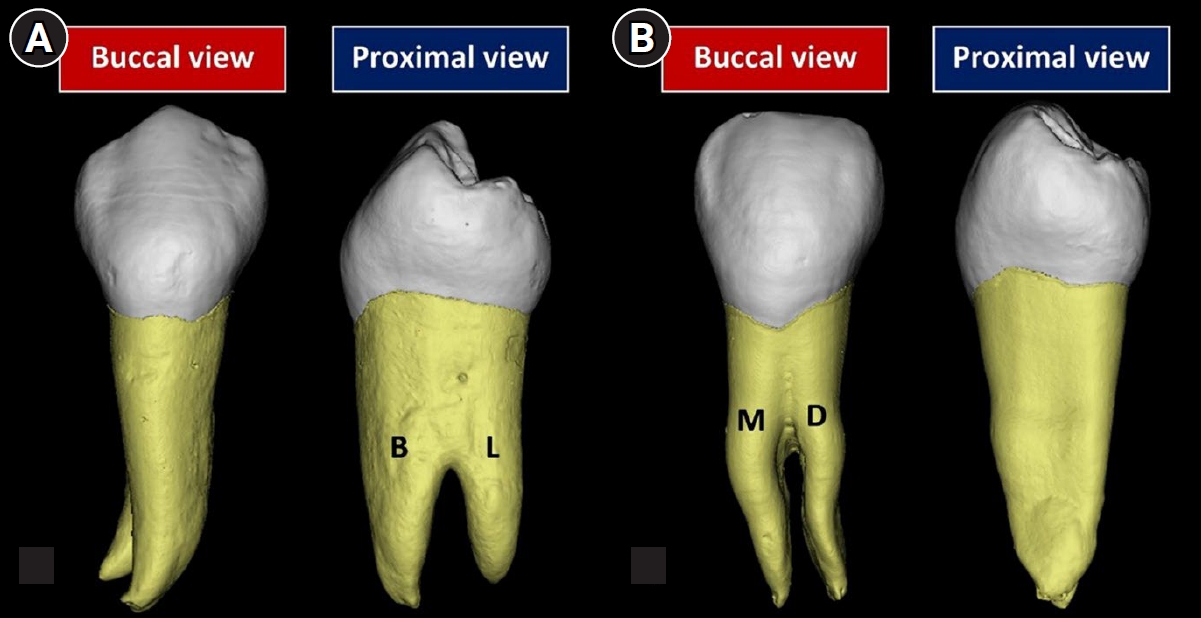
Micro-computed tomography reconstructed images of double-rooted mandibular premolars with (A) buccal and lingual roots and (B) mesial and distal roots. B, buccal; L, lingual; M, mesial; D, distal. Reproduced from Ahmed et al. [10], according to the Creative Commons License.
Figure 5.
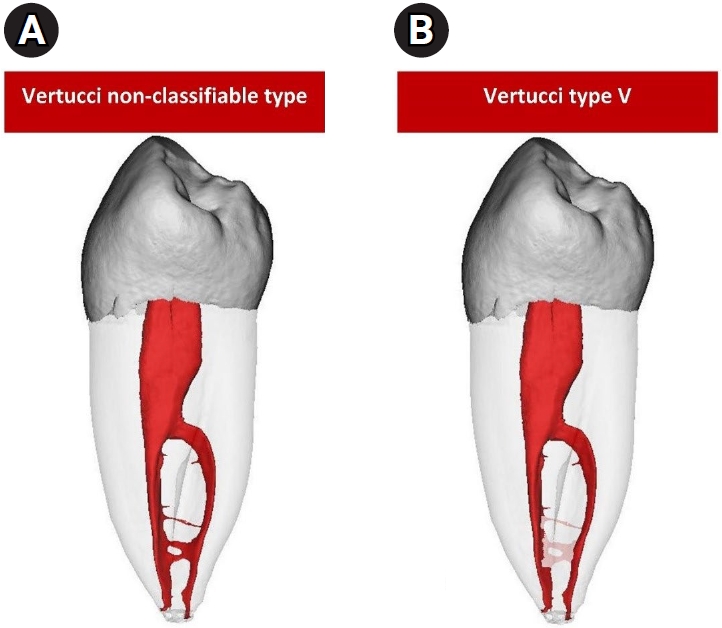
A micro-computed tomography image of a mandibular right first premolar, classified using the Vertucci classification [3]: (A) when intercanal communication is included, Vertucci non-classifiable (1-2-1-2-1-2-1-2); (B) when intercanal communication is not included, Vertucci type V.
Figure 6.
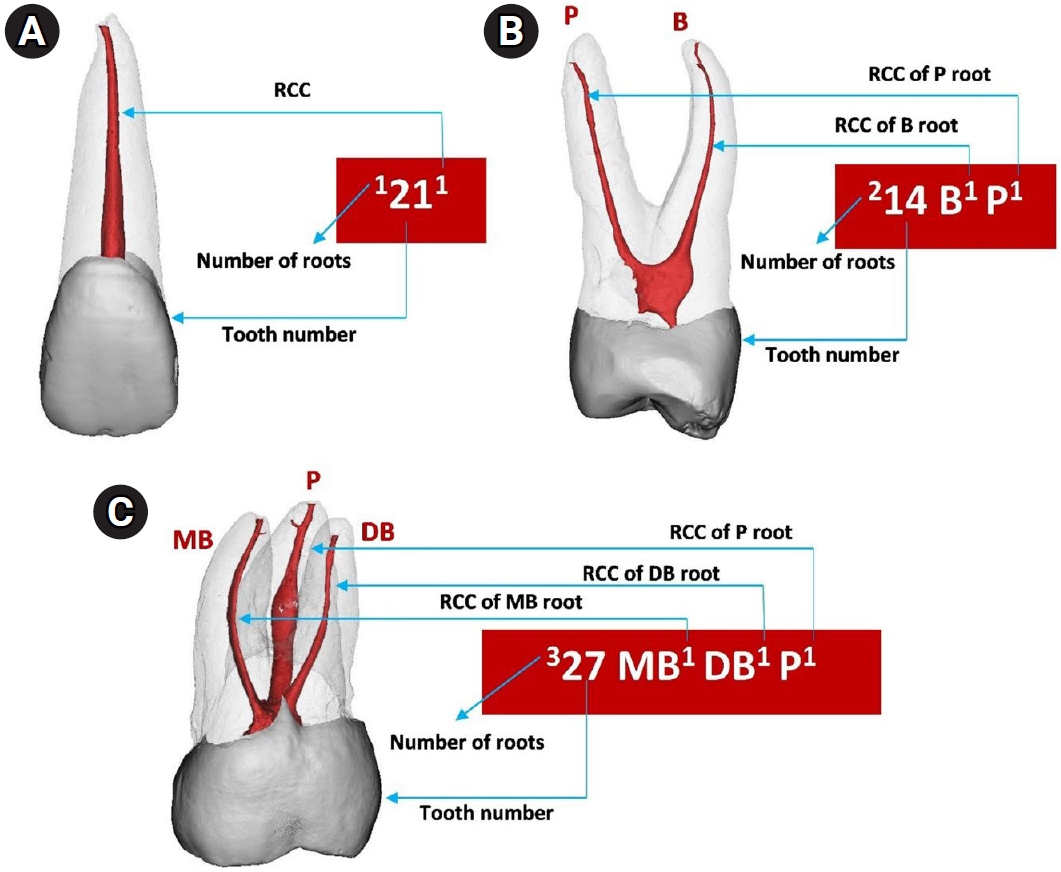
Micro-computed tomography reconstructed images showing the application of the Ahmed et al.’s coding system [9] in a range of teeth. (A) 1211 refers to a single rooted tooth 21 with a single root canal configuration, (B) 214 B1 P1 refers to a double-rooted tooth 14 in which each of the B and P roots has one root canal, (C) 327 MB1 DB1 P1 refers to a three-rooted tooth 27 in which each of the MB, DB and P roots has a single root canal configuration. RCC, root canal configuration; P, palatal; B, buccal; MB, mesio-buccal; DB, disto-buccal.
Figure 7.
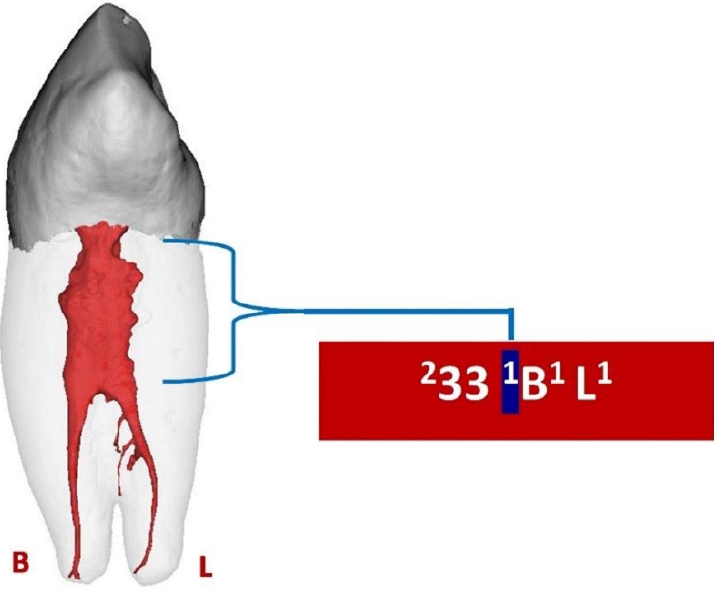
Three-dimensional reconstructed double-rooted mandibular canine with a common canal coronally identified by a superscript number (highlighted in blue) before the buccal (B) and lingual (L) roots.
Figure 8.
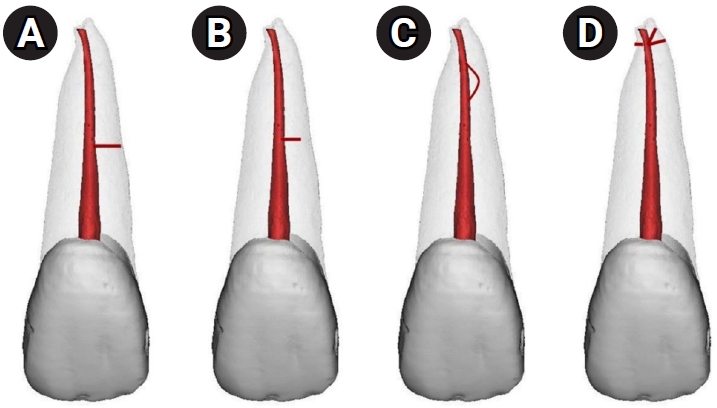
Application of the Ahmed et al.’ system [9] to classify root canal configuration and accessory canals in a single code. (A) 1211(M1): Single-rooted tooth 21 with one canal and one patent accessory canal in the middle third. (B) 1211(M1-0): Single-rooted tooth 21 with one canal and one blind accessory canal in the middle third. (C) 1211(M2-1-0): Single-rooted tooth 21 with one canal and one loop accessory canal in the middle third. (D) 1211(MD): Single-rooted tooth 21 with one canal and apical delta.
Figure 9.
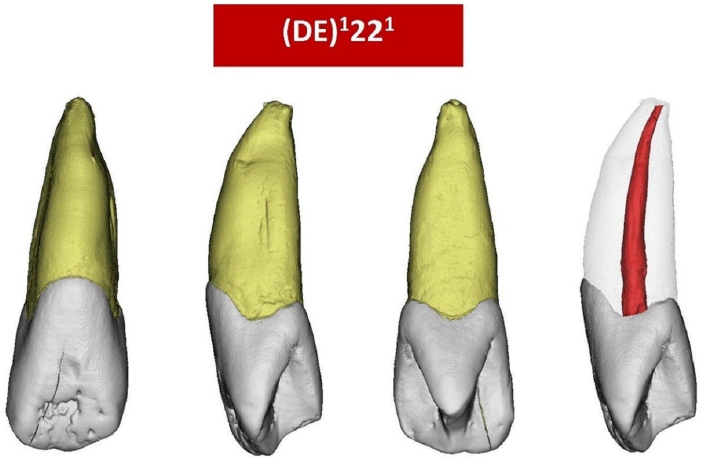
Application of the Ahmed et al.’ system [9] to classify a maxillary left lateral incisor with dens evaginatus (DE).
Figure 10.
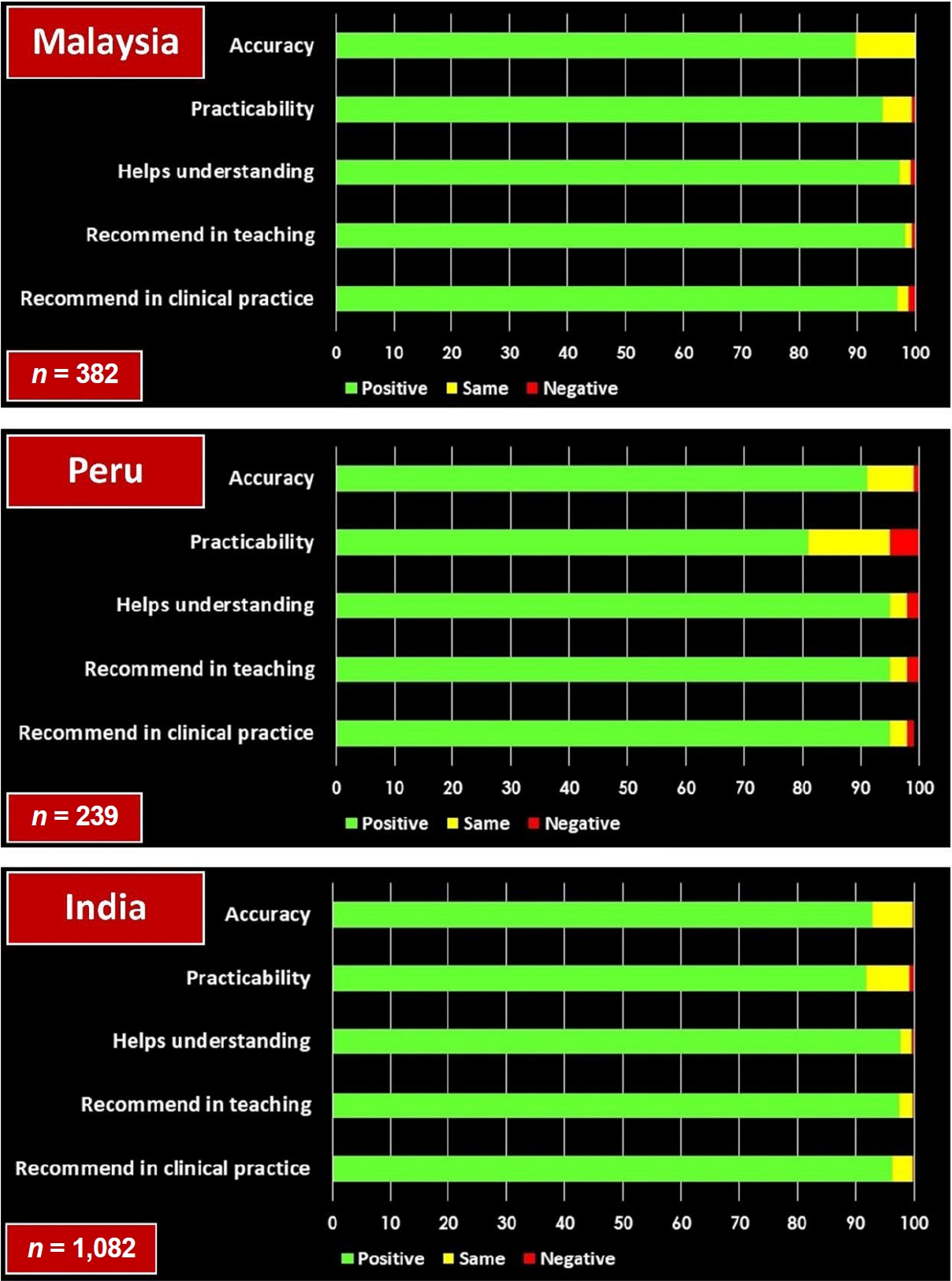
Summary of the results obtained from the three surveys that compared the feedback from students and dentists on the Ahmed et al.’ coding system [9] compared to the Vertucci classification [3] in terms of accuracy, practicability, help in understanding of root canal anatomy, and recommendations in teaching and clinical practice.
Figure 11.

Potential application of micro-computed tomography (micro-CT) scanned teeth for virtual reality (VR) applications using complementary codes of the Ahmed et al.’s system [9]. (A) After micro-CT scanning (axial section) and the use of Mimics software (DICOM files). (B) After segmentation of the enamel, dentine, and pulp space. (C) After three-dimensional (3D) reconstruction. (D) Conversion to STL (Standard Tessellation Language) files. (E) Using Blender (version 4.4.3; Blender Foundation, Amsterdam, Netherlands) for 3D reconstruction. (F) After the addition of complementary codes for main and accessory canals for a single-rooted tooth 42 with canal configuration 1-2-1 and an apical delta (D). This can be used with a VR device.
Table 1.
A list of the survey studies that examined the preference of students when using the Ahmed et al. coding system [9]
| Study | Year | Country | Teaching method used | Participants | Types of questions | Criteria of the presenter(s) |
|---|---|---|---|---|---|---|
| Ahmed et al. [44] | 2020 | Malaysia | PowerPoint presentation (physical lecture) (English) | Undergraduates (n = 382) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | Two calibrated presenters graduated from a dental school not less than 10 years ago, had at least 3 years of teaching experience, and did not contribute to the development of the classification systems involved |
| Salas et al. [45] | 2021 | Peru | PowerPoint presentation (online lecture) (Spanish) | General dental practitioners and endodontic specialists (82%), members of the Peru Society of Endodontics and dental students (18%) (n = 239) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | The presentation was delivered by the first author in an online lecture |
| Karobari et al. [46] | 2023 | India | PowerPoint presentation (physical and online lecture) (English) | Undergraduates, interns, and postgraduates (n = 1,082) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | A trained and calibrated presenter who did not contribute to the development of the classification systems involved |
| Pérez-Higueras et al. [47] | 2024 | Spain | PowerPoint presentation (physical lecture followed by a seminar) (Spanish) | Undergraduates (n = 81) | Multi-choice questions (n = 6) followed by open-ended questions (n = 2) | A facilitator with teaching experience in undergraduate endodontics of at least 10 years |
| The students were then divided into small groups (10–12 each) |
- 1. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3-29.Article
- 2. Hess W, Zürcher E. The anatomy of the root-canals of the teeth of the permanent dentition. New York: William Wood & Co; 1925.
- 3. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589-599.ArticlePubMed
- 4. Weine FS, Hayami S, Hata G, Toda T. Canal configuration of the mesiobuccal root of the maxillary first molar of a Japanese sub-population. Int Endod J 1999;32:79-87.ArticlePubMed
- 5. Morfis A, Sylaras SN, Georgopoulou M, Kernani M, Prountzos F. Study of the apices of human permanent teeth with the use of a scanning electron microscope. Oral Surg Oral Med Oral Pathol 1994;77:172-176.ArticlePubMed
- 6. Martins JN, Marques D, Mata A, Caramês J. Root and root canal morphology of the permanent dentition in a Caucasian population: a cone-beam computed tomography study. Int Endod J 2017;50:1013-1026.ArticlePubMedPDF
- 7. Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Arch Oral Biol 2016;61:130-137.ArticlePubMed
- 8. Stains M, Talanquer V. Classification of chemical reactions: stages of expertise. J Res Sci Teaching 2008;45:771-793.Article
- 9. Ahmed HM, Versiani MA, De-Deus G, Dummer PM. A new system for classifying root and root canal morphology. Int Endod J 2017;50:761-770.ArticlePubMedPDF
- 10. Ahmed HM, Rossi-Fedele G, Dummer PM. Critical analysis of a new system to classify root and canal morphology: a systematic review. Aust Endod J 2023;49:750-768.ArticlePubMed
- 11. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol 1969;28:419-425.ArticlePubMed
- 12. Vertucci F, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol 1974;38:456-464.ArticlePubMed
- 13. Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001;34:359-370.ArticlePubMedPDF
- 14. Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J 2002;35:56-62.ArticlePubMed
- 15. Ng YL, Aung TH, Alavi A, Gulabivala K. Root and canal morphology of Burmese maxillary molars. Int Endod J 2001;34:620-630.ArticlePubMedPDF
- 16. Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30:391-398.ArticlePubMed
- 17. Versiani MA, Ordinola-Zapata R. Root canal anatomy: implications in biofilm disinfection. In: Chávez de Paz L, Sedgley C, Kishen A, editors. Root canal biofilms. Cham: Springer; 2015.
- 18. Ahmed HM, Hashem AA, Dummer PM. Application of a new system for classifying root and canal anatomy in clinical practice: explanation and elaboration. Eur Endod J 2021;6:132-142.ArticlePubMedPMCPDF
- 19. Ahmed HM, Cheung GS. Accessory roots and root canals in maxillary premolar teeth: a review of a critical endodontic challenge. ENDO (Lond Engl) 2012;6:7-18.
- 20. Ahmed HM, Hashem AA. Accessory roots and root canals in human anterior teeth: a review and clinical considerations. Int Endod J 2016;49:724-736.ArticlePubMed
- 21. Neelakantan P, Subbarao C, Ahuja R, Subbarao CV. Root and canal morphology of Indian maxillary premolars by a modified root canal staining technique. Odontology 2011;99:18-21.ArticlePubMedPDF
- 22. Ahmed HM, Ibrahim N, Mohamad NS, Nambiar P, Muhammad RF, Yusoff M, et al. Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography: explanation and elaboration. Int Endod J 2021;54:1056-1082.ArticlePubMedPDF
- 23. Ahmed HM, Keleş A, Wolf TG, Nagendrababu V, Duncan HF, Peters OA, et al. Controversial terminology in root and canal anatomy: a comprehensive review. Eur Endod J 2024;9:308-334.ArticlePubMedPMCPDF
- 24. American Association of Endodontists. Glossary of endodontic terms [Internet]. Chicago: American Association of Endodontists; 2020 [cited 2024 Oct 18]. Available from: https://www.aae.org/specialty/download/glossary-of-endodontic-terms/
- 25. Karobari MI, Noorani TY, Halim MS, Dummer PM, Ahmed HM. Should inter-canal communications be included in the classification of root canal systems? Int Endod J 2019;52:917-919.ArticlePubMedPDF
- 26. Filpo-Perez C, Bramante CM, Villas-Boas MH, Húngaro Duarte MA, Versiani MA, Ordinola-Zapata R. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J Endod 2015;41:231-236.ArticlePubMed
- 27. Leoni GB, Versiani MA, Pécora JD, Damião de Sousa-Neto M. Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod 2014;40:710-716.Article
- 28. Arslan H, Ertas H, Ertas ET, Kalabalık F, Saygılı G, Capar ID. Evaluating root canal configuration of mandibular incisors with cone-beam computed tomography in a Turkish population. J Dent Sci 2015;10:359-364.Article
- 29. da Silva EJ, de Castro RW, Nejaim Y, Silva AI, Haiter-Neto F, Silberman A, et al. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: an in-vivo study. Quintessence Int 2016;47:19-24.ArticlePubMed
- 30. von Arx T. Frequency and type of canal isthmuses in first molars detected by endoscopic inspection during periradicular surgery. Int Endod J 2005;38:160-168.ArticlePubMed
- 31. Endal U, Shen Y, Knut A, Gao Y, Haapasalo M. A high-resolution computed tomographic study of changes in root canal isthmus area by instrumentation and root filling. J Endod 2011;37:223-227.ArticlePubMed
- 32. Wu MK, Dummer PM, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. Int Endod J 2006;39:343-356.ArticlePubMed
- 33. Villegas JC, Yoshioka T, Kobayashi C, Suda H. Frequency of transverse anastomoses with and without apical communication in Japanese population teeth. Aust Endod J 2004;30:50-52.ArticlePubMed
- 34. Verma P, Love RM. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J 2011;44:210-217.ArticlePubMed
- 35. Lee KW, Kim Y, Perinpanayagam H, Lee JK, Yoo YJ, Lim SM, et al. Comparison of alternative image reformatting techniques in micro-computed tomography and tooth clearing for detailed canal morphology. J Endod 2014;40:417-422.ArticlePubMed
- 36. Kim Y, Chang SW, Lee JK, Chen IP, Kaufman B, Jiang J, et al. A micro-computed tomography study of canal configuration of multiple-canalled mesiobuccal root of maxillary first molar. Clin Oral Investig 2013;17:1541-1546.ArticlePubMedPDF
- 37. Ahmed HM, Musale PK, El Shahawy OI, Dummer PM. Application of a new system for classifying tooth, root and canal morphology in the primary dentition. Int Endod J 2020;53:27-35.ArticlePubMedPDF
- 38. Oehlers FA. Dens invaginatus (dilated composite odontome): I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957;10:1204-1218.
- 39. Oehlers FA. Dens invaginatus (dilated composite odontome): II. Associated posterior crown forms and pathogenesis. Oral Surg Oral Med Oral Pathol 1957;10:1302-1316.ArticlePubMed
- 40. Cantatore G, Berutti E, Castellucci A. Missed anatomy: frequency and clinical impact. Endod Top 2006;15:3-31.Article
- 41. Ahmed HM, El-Karim I, Duncan HF, Krastl G, Galler K. Implications of root, pulp chamber, and canal anatomy on pulpotomy and revitalization procedures. Clin Oral Investig 2023;27:6357-6369.ArticlePubMedPDF
- 42. Lydeard S. The questionnaire as a research tool. Fam Pract 1991;8:84-91.ArticlePubMed
- 43. Mala S, Lynch CD, Burke FM, Dummer PM. Attitudes of final year dental students to the use of rubber dam. Int Endod J 2009;42:632-638.ArticlePubMed
- 44. Ahmed HM, Che Ab Aziz ZA, Azami NH, Farook MS, Khan AA, Mohd Noor NS, et al. Application of a new system for classifying root canal morphology in undergraduate teaching and clinical practice: a national survey in Malaysia. Int Endod J 2020;53:871-879.ArticlePubMedPDF
- 45. Salas H, Torres J, Pauro J, Ahmed HM. A new coding system for root and canal morphology: an online survey from Peru. Int Endod J 2021;54:147-149.ArticlePubMedPDF
- 46. Karobari MI, Ahmed HM, Khamis MF, Ibrahim N, Noorani TY. Application of two systems to classify the root and canal morphology in the human dentition: a national survey in India. J Dent Educ 2023;87:1089-1098.ArticlePubMed
- 47. Pérez-Higueras JJ, Oteo B, Gancedo-Caravia L, Arias A. Influence of the incorporation of small-group practical seminars to a traditional lecture for the understanding of root canal morphology classification systems. Eur J Dent Educ 2024;28:371-376.ArticlePubMed
- 48. Krathwohl DR. A revision of Bloom’s taxonomy: an overview. Theory Pract 2002;41:212-218.Article
- 49. Aljawhar AM, Ibrahim N, Abdul Aziz A, Ahmed HM, Azami NH. Micro-computed tomographic evaluation of root and canal anatomy of maxillary first premolars in Iraqi sub-population. Sci Rep 2025;15:10821.ArticlePubMedPMCPDF
- 50. Ahmed HM, Noor NS, Hasanusi HF, Khalid PN, Nabhan MS, Noorani TY, et al. Characterisation of root canal configurations and accessory canals in mandibular incisors: a micro-computed tomography study on a Malaysian subpopulation. Aust Endod J 2025;51:258-266.ArticlePubMed
- 51. Villa N, Weissheimer T, Vier-Pelisser FV, Alcalde MP, Vivan RR, Duarte MA, et al. Comparative study of Vertucci and Ahmed classifications to evaluate the main root canal configuration of mandibular incisors in a Brazilian population. Aust Endod J 2022;48:409-414.ArticlePubMedPDF
- 52. Saber SM, Elashiry MM, Sadat SM, Nawar NN. A microcomputed tomographic analysis of the morphological variabilities and incidence of extra canals in mandibular first molar teeth in an Egyptian subpopulation. Sci Rep 2023;13:8985.ArticlePubMedPMCPDF
- 53. Olczak K, Pawlicka H, Szymański W. Root form and canal anatomy of maxillary first premolars: a cone-beam computed tomography study. Odontology 2022;110:365-375.ArticlePubMedPDF
- 54. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, van Schoor A, Uys A. A study of mandibular premolar root and canal morphology in a Black South African population using cone-beam computed tomography and two classification systems. J Oral Sci 2022;64:300-306.ArticlePubMed
- 55. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, Van Schoor A, Uys A. Root and canal morphology of maxillary second molars in a Black South African subpopulation using cone-beam computed tomography and two classifications. Aust Endod J 2023;49 Suppl 1:217-227.ArticlePubMedPDF
- 56. Pertek Hatipoğlu F, Magat G, Karobari MI, Madarati AA, Tulegenova I, Hatipoğlu Ö, et al. Root and canal configurations of maxillary first premolars in 22 countries using two classification systems: a multinational cross-sectional study. Sci Rep 2025;15:19290.ArticlePubMedPMC
- 57. Ahmed HM. A critical analysis of laboratory and clinical research methods to study root and canal anatomy. Int Endod J 2022;55 Suppl 2:229-280.ArticlePubMedPDF
- 58. Reymus M, Liebermann A, Diegritz C. Virtual reality: an effective tool for teaching root canal anatomy to undergraduate dental students: a preliminary study. Int Endod J 2020;53:1581-1587.ArticlePubMedPDF
- 59. Diegritz C, Fotiadou C, Fleischer F, Reymus M. Tooth anatomy inspector: a comprehensive assessment of an extended reality (XR) application designed for teaching and learning of root canal anatomy by students. Int Endod J 2024;57:1682-1688.ArticlePubMed
- 60. Ahmed HM, Al-Maswary A, Habaebi M, Tasdelen A, Al Husaini MA, Elnawawy H, et al. Artificial intelligence in the study of root and canal anatomy: a comprehensive review on applications, advantages, challenges and future directions. Eur Endod J 2025;10:343-364.ArticlePubMedPMCPDF
- 61. Aminoshariae A, Nosrat A, Nagendrababu V, Dianat O, Mohammad-Rahimi H, O'Keefe AW, et al. Artificial intelligence in endodontic education. J Endod 2024;50:562-578.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteEducational implications of a novel system for classifying root and canal anatomy in the human dentition: a narrative review
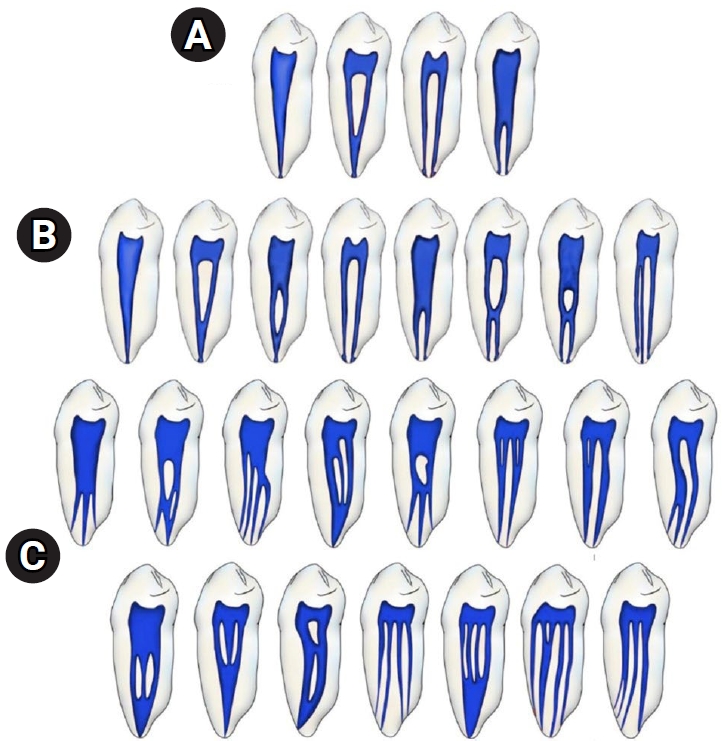
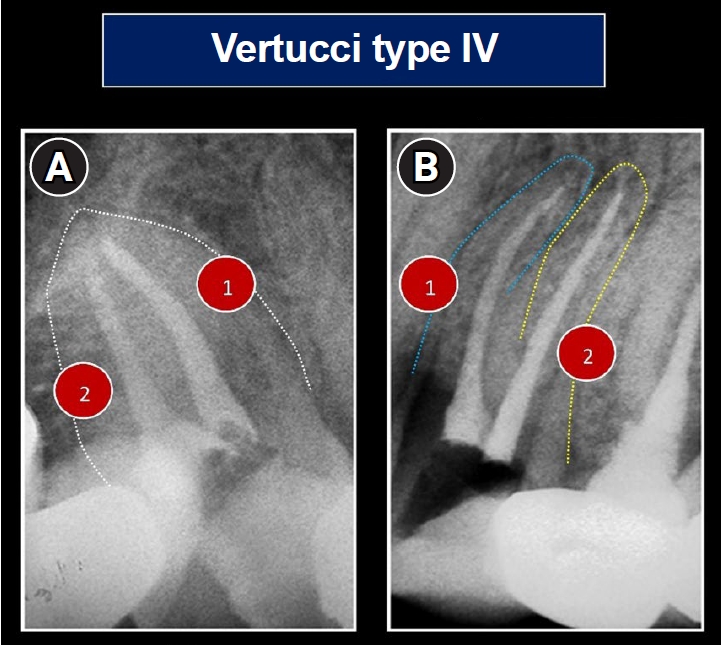
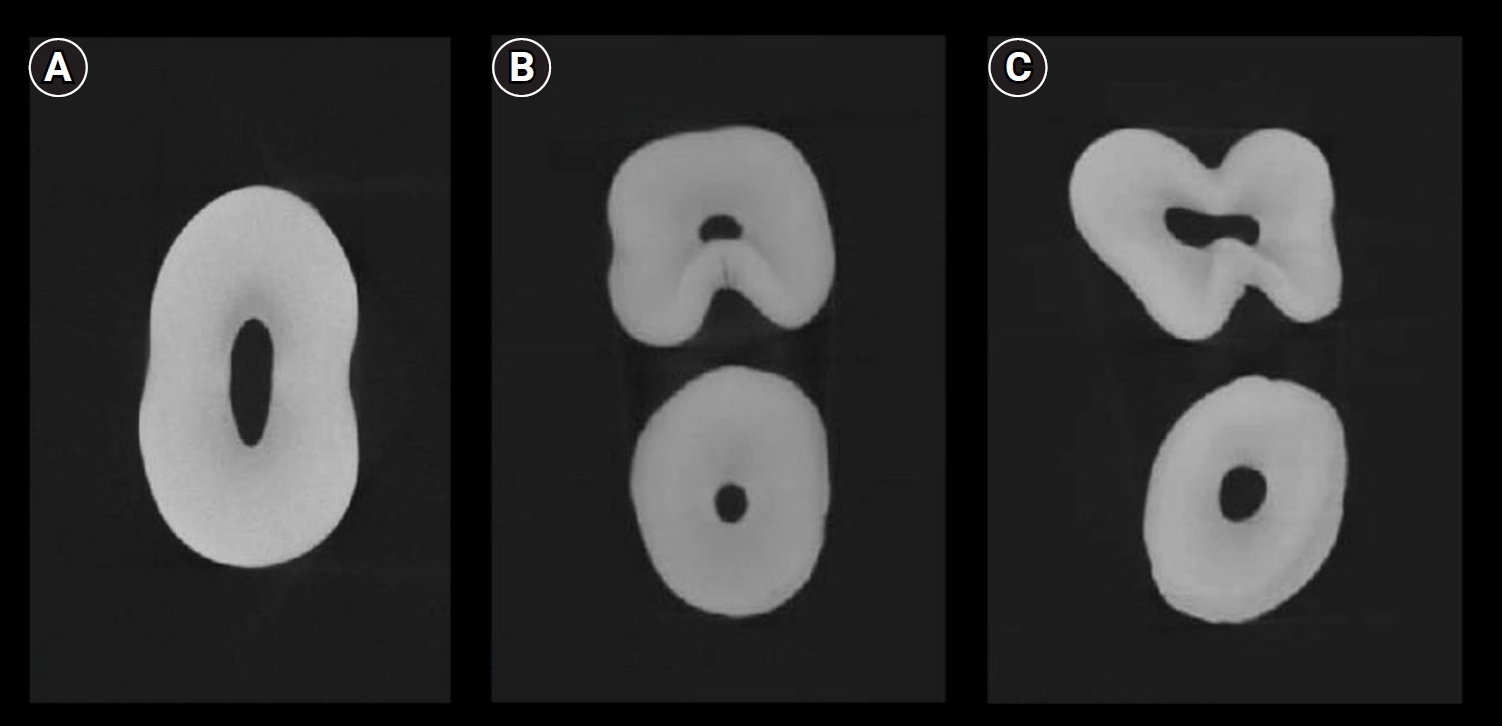
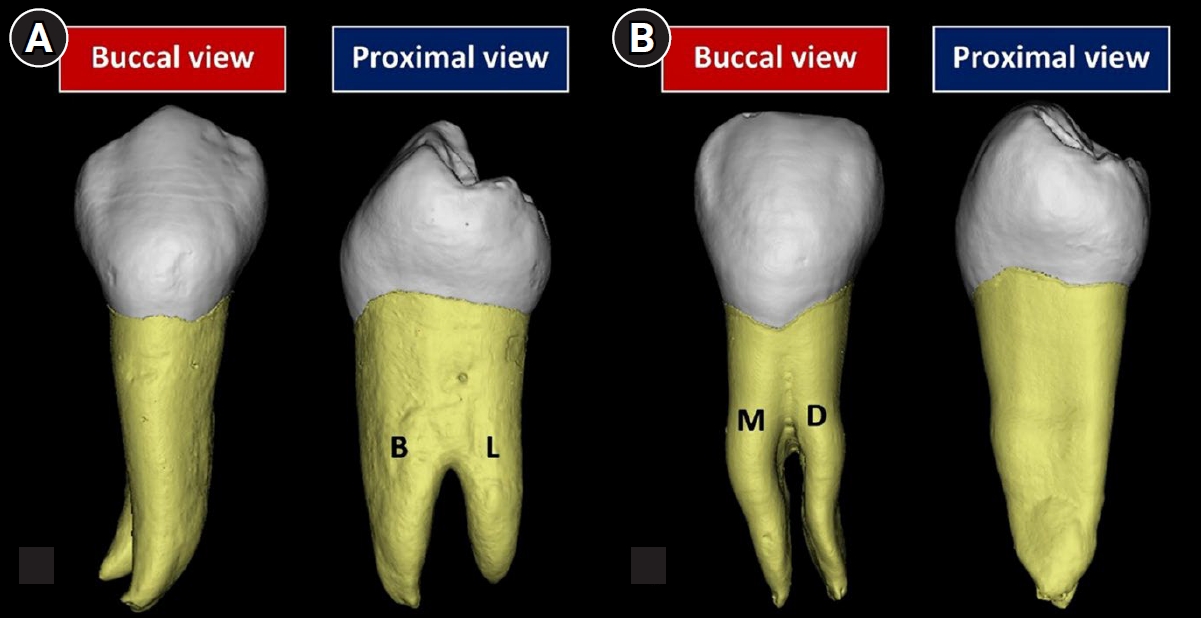
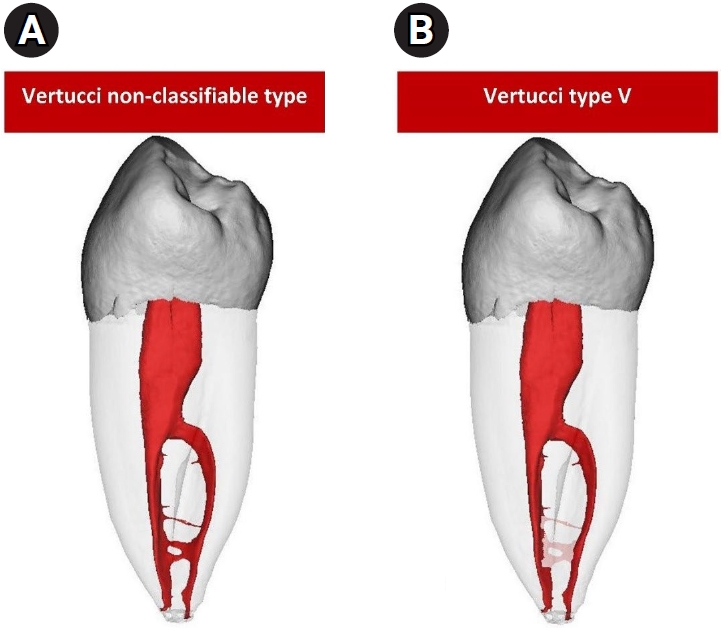
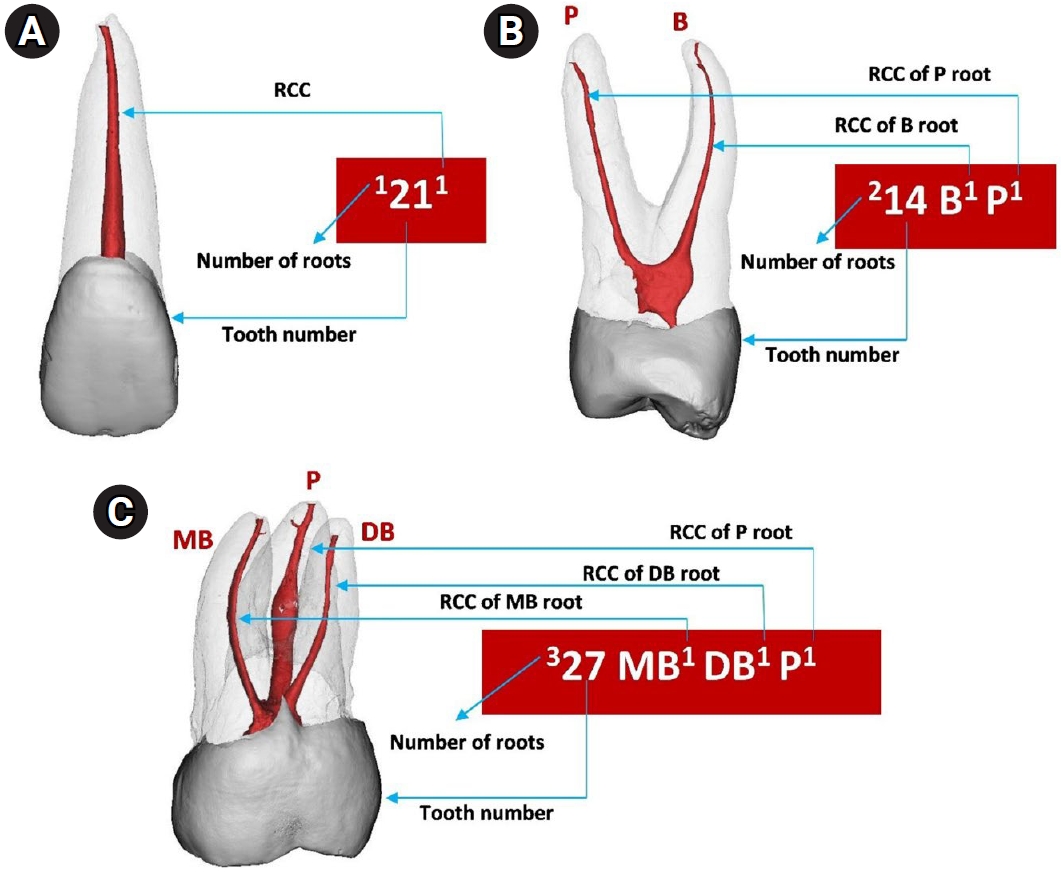
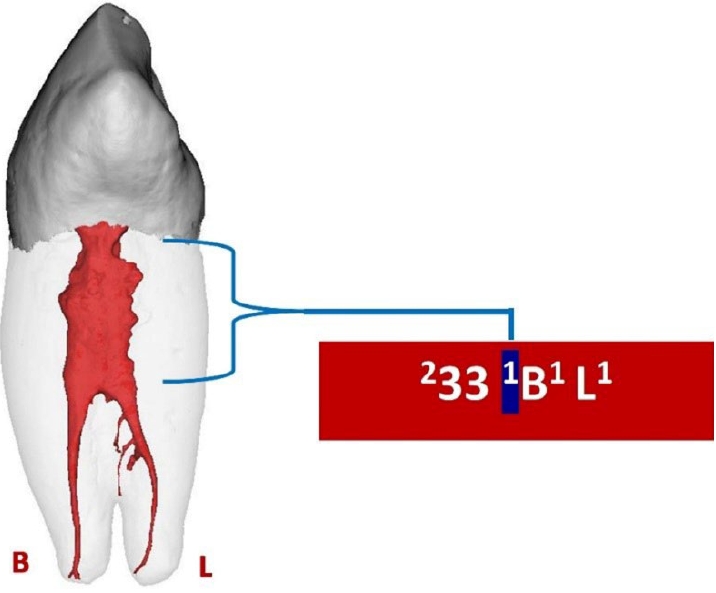
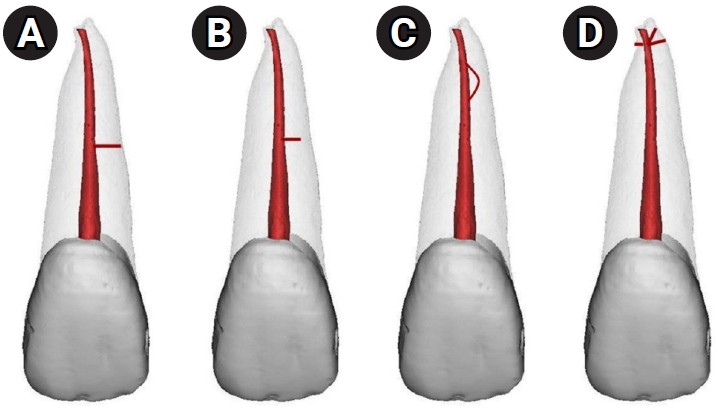
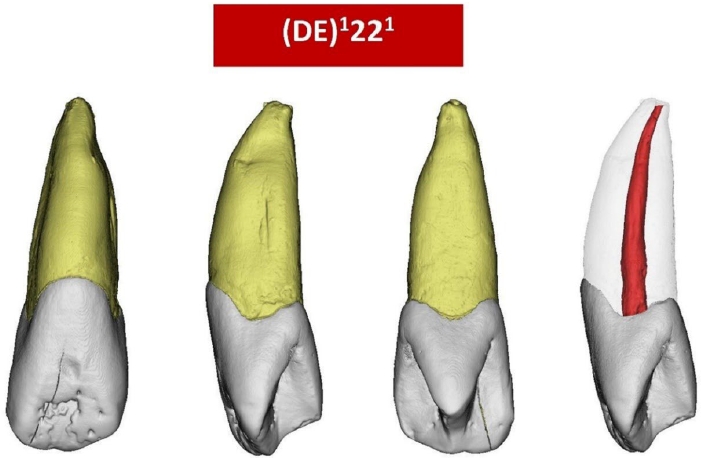

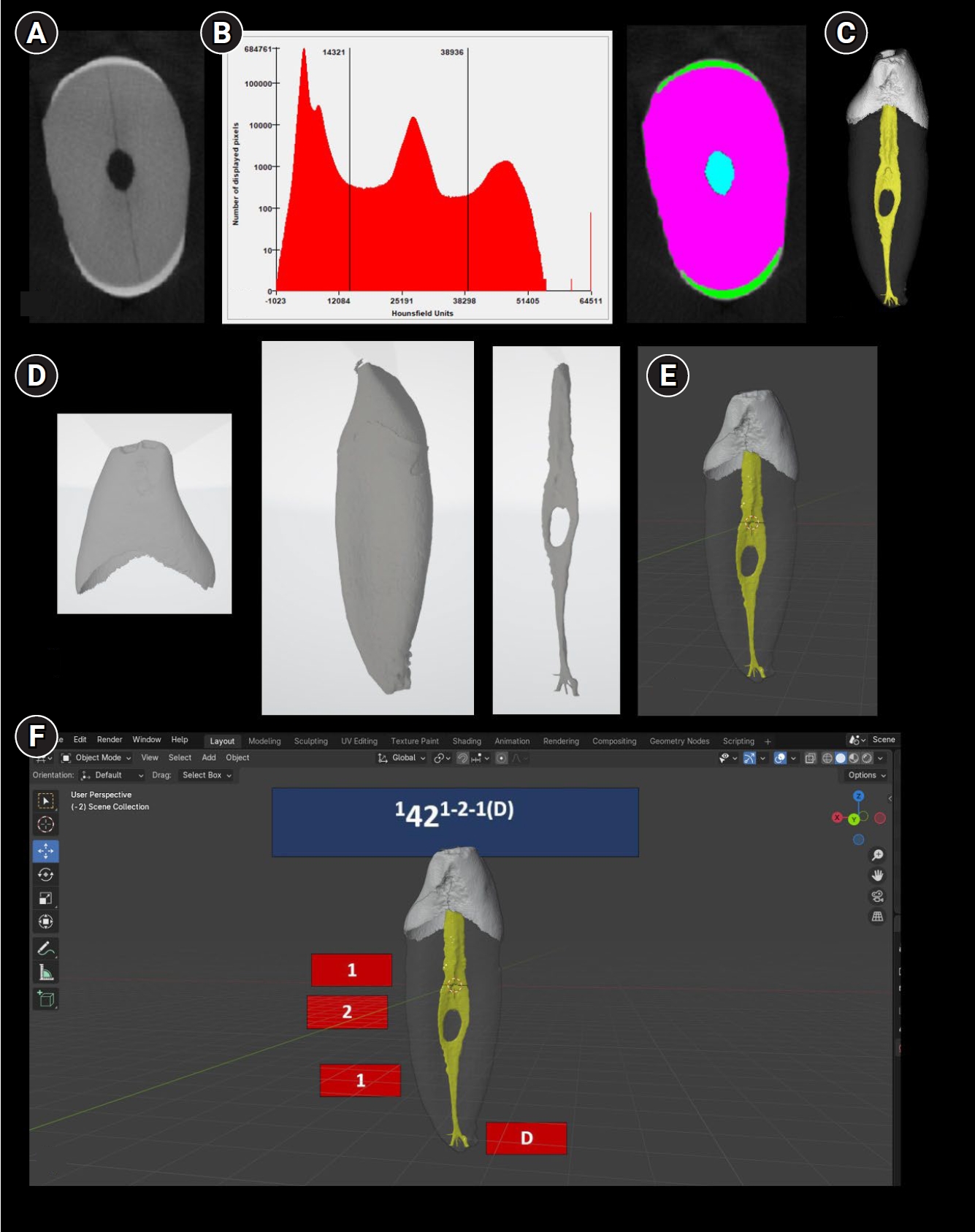
Figure 1. Common classifications of root canal configurations. (A) Weine et al.’s classification [11]: types I (1), II (2-1), III (2), and IV (1-2). (B) Vertucci et al.’s classification [12]: types I (1), II (2-1), III (1-2-1), IV (2), V (1-2), VI (2-1-2), VII (1-2-1-2), and VIII (3). (C) Supplemental configurations of the Vertucci classification [13–16]: types IX (1-3), X (1-2-3-2), XI (1-2-3-4), XII (2-3-1), XIII (1-2-1-3), XIV (4-2), XV (3-2), XVI (2-3), XVII (1-3-1), XVIII (3-1), XIX (2-1-2-1), XX (4), XXI (4-1), XXII (5-4), and XXIII (3-4).
Figure 2. Periapical radiographs of a single-rooted (A) and double-rooted (B) maxillary premolar which are classified the same using the Vertucci classification, that is, type IV (two separate canals). Reproduced and modified from Ahmed et al. [18], according to the Creative Commons License.
Figure 3. Micro-computed tomography images showing the morphological variations in the axial sections of maxillary premolars: (A) single-rooted; (B) double-rooted with a furcation groove in the palatal aspect of the buccal root; and (C) double-rooted with developmental grooves in the buccal and palatal aspects of the root.
Figure 4. Micro-computed tomography reconstructed images of double-rooted mandibular premolars with (A) buccal and lingual roots and (B) mesial and distal roots. B, buccal; L, lingual; M, mesial; D, distal. Reproduced from Ahmed et al. [10], according to the Creative Commons License.
Figure 5. A micro-computed tomography image of a mandibular right first premolar, classified using the Vertucci classification [3]: (A) when intercanal communication is included, Vertucci non-classifiable (1-2-1-2-1-2-1-2); (B) when intercanal communication is not included, Vertucci type V.
Figure 6. Micro-computed tomography reconstructed images showing the application of the Ahmed et al.’s coding system [9] in a range of teeth. (A) 1211 refers to a single rooted tooth 21 with a single root canal configuration, (B) 214 B1 P1 refers to a double-rooted tooth 14 in which each of the B and P roots has one root canal, (C) 327 MB1 DB1 P1 refers to a three-rooted tooth 27 in which each of the MB, DB and P roots has a single root canal configuration. RCC, root canal configuration; P, palatal; B, buccal; MB, mesio-buccal; DB, disto-buccal.
Figure 7. Three-dimensional reconstructed double-rooted mandibular canine with a common canal coronally identified by a superscript number (highlighted in blue) before the buccal (B) and lingual (L) roots.
Figure 8. Application of the Ahmed et al.’ system [9] to classify root canal configuration and accessory canals in a single code. (A) 1211(M1): Single-rooted tooth 21 with one canal and one patent accessory canal in the middle third. (B) 1211(M1-0): Single-rooted tooth 21 with one canal and one blind accessory canal in the middle third. (C) 1211(M2-1-0): Single-rooted tooth 21 with one canal and one loop accessory canal in the middle third. (D) 1211(MD): Single-rooted tooth 21 with one canal and apical delta.
Figure 9. Application of the Ahmed et al.’ system [9] to classify a maxillary left lateral incisor with dens evaginatus (DE).
Figure 10. Summary of the results obtained from the three surveys that compared the feedback from students and dentists on the Ahmed et al.’ coding system [9] compared to the Vertucci classification [3] in terms of accuracy, practicability, help in understanding of root canal anatomy, and recommendations in teaching and clinical practice.
Figure 11. Potential application of micro-computed tomography (micro-CT) scanned teeth for virtual reality (VR) applications using complementary codes of the Ahmed et al.’s system [9]. (A) After micro-CT scanning (axial section) and the use of Mimics software (DICOM files). (B) After segmentation of the enamel, dentine, and pulp space. (C) After three-dimensional (3D) reconstruction. (D) Conversion to STL (Standard Tessellation Language) files. (E) Using Blender (version 4.4.3; Blender Foundation, Amsterdam, Netherlands) for 3D reconstruction. (F) After the addition of complementary codes for main and accessory canals for a single-rooted tooth 42 with canal configuration 1-2-1 and an apical delta (D). This can be used with a VR device.
Figure 1.
Figure 2.
Figure 3.
Figure 4.
Figure 5.
Figure 6.
Figure 7.
Figure 8.
Figure 9.
Figure 10.
Figure 11.
Educational implications of a novel system for classifying root and canal anatomy in the human dentition: a narrative review
| Study | Year | Country | Teaching method used | Participants | Types of questions | Criteria of the presenter(s) |
|---|---|---|---|---|---|---|
| Ahmed et al. [44] | 2020 | Malaysia | PowerPoint presentation (physical lecture) (English) | Undergraduates (n = 382) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | Two calibrated presenters graduated from a dental school not less than 10 years ago, had at least 3 years of teaching experience, and did not contribute to the development of the classification systems involved |
| Salas et al. [45] | 2021 | Peru | PowerPoint presentation (online lecture) (Spanish) | General dental practitioners and endodontic specialists (82%), members of the Peru Society of Endodontics and dental students (18%) (n = 239) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | The presentation was delivered by the first author in an online lecture |
| Karobari et al. [46] | 2023 | India | PowerPoint presentation (physical and online lecture) (English) | Undergraduates, interns, and postgraduates (n = 1,082) | Multi-choice questions (n = 5) followed by an open-ended question (n = 1) | A trained and calibrated presenter who did not contribute to the development of the classification systems involved |
| Pérez-Higueras et al. [47] | 2024 | Spain | PowerPoint presentation (physical lecture followed by a seminar) (Spanish) | Undergraduates (n = 81) | Multi-choice questions (n = 6) followed by open-ended questions (n = 2) | A facilitator with teaching experience in undergraduate endodontics of at least 10 years |
| The students were then divided into small groups (10–12 each) |
Table 1. A list of the survey studies that examined the preference of students when using the Ahmed et al. coding system [9]

