
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 36(1); 2011 > Article
- Case Report Management of white spots: resin infiltration technique and microabrasion
- Jeong-Hye Son, DDS, MS, Bock Hur, DDS, PhD, Hyeon-Cheol Kim, DDS, PhD, Jeong-Kil Park, DDS, PhD
-
2011;36(1):-71.
DOI: https://doi.org/10.5395/JKACD.2011.36.1.66
Published online: January 31, 2011
Department of Conservative Dentistry, Pusan National University School of Dentistry, Yangsan, Korea.
- Correspondence to Jeong-Kil Park, DDS, PhD. Associate Professor, Department of Conservative Dentistry, Pusan National University School of Dentistry, Beomeo-ri, Mulgem, Yangsan, Korea 626-770. TEL, +82-55-360-5213; FAX, +82-55-360-5214; jeongkil@pusan.ac.kr
• Received: November 2, 2010 • Revised: November 23, 2010 • Accepted: November 25, 2010
Copyright © 2011 Korean Academy of Conservative Dentistry
- 5,893 Views
- 50 Download
- 25 Crossref
Abstract
- This case report compared the effectiveness of resin infiltration technique (Icon, DMG) with microabrasion (Opalustre, Ultradent Products, Inc.) in management of white spot lesions. It demonstrates that although neither microabrasion nor resin infiltration technique can remove white spot lesions completely, resin infiltration technique seems to be more effective than microabrasion. Therefore resin infiltration technique can be chosen preferentially for management of white spot lesions and caution should be taken for case selection.
Introduction
White spot lesions are defined as the enamel lesions that look chalky white and opaque. It can arise from developmental cause such as fluorosis, idiopathic cause or early caries lesion. Incipient caries, one of the white spot lesions, is the enamel caries lesion that can be clinically recognized for the first time.
White spot lesions develop as a result of a dietary carbohydrate and saliva modified bacterial infection, resulting in an imbalance between demineralization and remineralization of the enamel.1,2 And these are generally considered to be the precursor of frank enamel carious lesions.3 The white appearance is due to an optical phenomenon which is caused by mineral loss in the surface or subsurface enamel. Enamel crystal dissolution begins with subsurface demineralization, creating pores between the enamel rods. The resultant alteration of the refractive index in the affected area is then a consequence of both surface roughness and loss of surface shine and alterations in internal reflection, all resulting in greater visual enamel opacity, as porous enamel scatters more light than sound enamel.4
In regard to the prevalence of white spot lesions, it has been reported that there is a significant increase in the prevalence and severity of enamel demineralization after orthodontic treatment.3 The overall prevalence of white spot lesions amongst orthodontic patients has been reported as anywhere between 2 and 96 percent.5 Some white spot lesions may remineralize and return either to normal or at last to a visually acceptable appearance. However, white spot lesions may also persist, resulting in an aesthetically unacceptable result.3
Several techniques have been proposed to improve the appearance of white spot lesions. The common treatment strategy for white spot lesions comprises restorative procedures, improvement of reminealization using CCP-ACP containing or fluoride containing products, microabrasion, argon-laser irradiation.6,7 Recently, 'resin infiltration technique' was introduced with the development of highly-flowable resin material. The following case report describes the effect of resin infiltration technique to mask white spots that was detected after debonding of fixed orthodontic appliance and calculus removal.
Case reports
After reading and receiving all necessary explanations including the experimental rationale, the clinical procedures and possible risk, the patients were asked to sign a consent form explaining the research protocol, which was previously approved by the Ethics Committee of Pusan National University Hospital Medical Research Institute (IRB, 2010092).
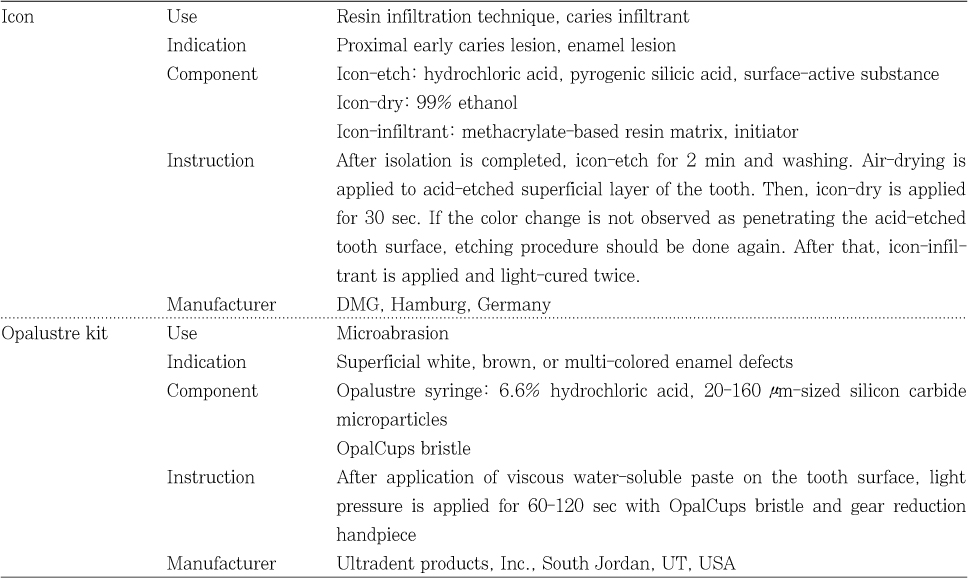
A 26-year-old female came to correct the white lesions on mandibular anterior teeth and premolars (Figures 1a, 2a, 3a). The patient's history included orthodontic treatment 10 years ago and the white spot lesions had existed since brackets were removed. Under the agreement, a decision was made to perform microabrasion with Opalustre (Ultradent Products, Inc., South Jordan, UT, USA) on the left side and resin infiltration technique with Icon (DMG, Hamburg, Germany) on the right side of mandibular teeth. The materials used are shown in Table 1.
After OpalDam (Ultradent Products, Inc.) and rubber dam were applied, microabrasion was performed on the left side first. The teeth looked chalky-whitish and the white spot lesions became more prominent than before (Figures 1b and 2b). Then resin infiltration was performed on the right side. The size of white spot lesion became smaller, however, somewhat was left (Figures 1b and 3b). Neither microabrasion nor resin infiltration technique can remove the white spot lesions completely. However, the lesions on the right side, resin infiltrated teeth, became smaller and the lesions on the left side, microabrased teeth, became more opaque. Therefore, white spot lesions on the microabrased teeth were more conspicuous after treatment.
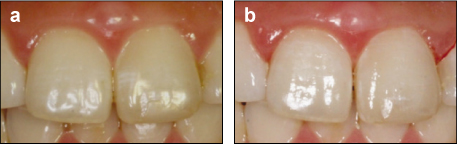
A 23-year-old female came with esthetic concern of anterior teeth (Figure 4a). Patient's history included orthodontic treatment 15 years ago. Because whitish lines on the maxillary right central incisor and white spot lesions on the maxillary left central incisor were detected (Figure 5a), fluoride varnish was applied periodically, but white spot lesions were not removed. Under the patient's agreement, a decision was made to perform microabrasion with Opalustre on maxillary right central incisor, resin infiltration technique with Icon on maxillary left central incisor and resin restoration on maxillary left lateral incisor. Whitish lines on the maxillary right central incisor which was treated by microabrasion became more whitish but the lesion on the maxillary left central incisor which was treated by resin infiltration technique looked smaller (Figures 4b and 5b). Even though some lesions are still left after treatment, resin infiltration technique seems more efficient with regard to the diminution of lesion size.
Discussion
White spot lesions are detected frequently and can be problematic for the patients with much esthetic concern. Several techniques have been proposed to improve the appearance of these white spot lesions. Among these, remineralization can be considered first for correct these white spot lesions. Because remineralization is a natural phenomenon resulting in the partial reversal of what is an early caries lesion. According to Willmote who studied the effect of fluoride and saliva after removal of fixed orthodontic appliance, the difference in percentage reduction of the white spot lesion size showed a reduction in lesion area of about a third after 12 week and a half after 26 weeks.8 However, remineralization of white spots takes a long time, and the lesions may be left to some degree. And it can inhibit the mineralization of subsurface lesions.
On the other hand, Ogaard et al. warned against treating visible white lesions on labial surfaces with concentrated fluoride agents, since this arrests the lesion (hypermineralization) and prevent complete repair.5 Especially deep lesions tend to remineralize only superficially. Consequently, arrested lesions show thick and highly mineralized surface layers.9 The underlying lesion body is still porous, however, and thus the whitish appearance often persists.10 Moreover, during remineralization stains can be incorporated into the lesion, leading to the formation of brown spots, a situation that might be judged as even more unesthetic.9 Therefore, some authors advocated allowing slow and gradual remineralization by saliva or low-concentrated fluoride agents such as fluoride mouth rinse and fluoride containing toothpaste on shallow lesion (< 60 µm), as this results in greater repair and less visible lesion.5
Enamel microabrasion was designed to improve the surface texture, remove the stains and recover remineralization. It removes superficial parts of the lesion by abrasion with a slurry of hydrochloric acid and pumice, and the enamel surface becomes smooth and glossy.10 Both chemical erosion with hydrochloric acid and mechanical abrasion with pumice simultaneously take place. Consequently, it uniformly removes up to 0.2 mm of enamel surface. According to Murphy et al. the mean reduction in white spot lesion size was 83%.11 Microabrasion can be applied for white spot lesion, fluorosis, demineralizarion after orthodontic treatment, localized hypoplasia, idiopathic hypoplasia. Donly et al. found that microabrasion re-created the outer, prism-free region and teeth became glassy and named 'abrosion effect'.12 This layer reflects or scatters the light and masks mild imperfections. However, substantial amounts of enamel often unfortunately have to be eroded to improve appearance with this technique.13
Resin infiltration technique is an alternative therapeutic approach to prevent further progression of enamel lesions. This treatment aims to occlude the microporosities within the lesion body by infiltration with low-viscosity light-curing resins that have been optimized for rapid penetration into the porous enamel.14 The resin penetrates into the lesion body, driven by capillary forces. This technique aims to create a diffusion barrier inside the lesion, not on the lesion surface. Robinson et al. reported that about 60 ± 10% of the lesion's pore volume had been occupied by resin.15 According to Kielbassa et al., resin infiltrates into subsurface lesions and produces resininfiltrated parts of the lesion.16 And the depth of resin infiltration was over 100 µm.
A positive side effect of resin infiltration is that enamel lesions lose their whitish appearance when their microporosities are filled with the resin and look similar to sound enamel. The principle of masking enamel lesions by resin infiltration is based on changes in light scattering within the lesions. Sound enamel has a refractive index (RI) of 1.62. The microporosities of enamel caries lesions are filled with either a watery medium (RI 1.33) or air (RI 1.0). The difference in refractive indices between the enamel crystals and medium inside the porosities causes light scattering that results in a whitish opaque appearance of these lesions, especially when they are desiccated.17 The microporosities of infiltrated lesions are filled with resin (RI 1.46) that, in contrast to the watery medium, cannot evaporate. Therefore, the difference in refractive indices between porosities and enamel is negligible and lesions appear similar to the surrounding sound enamel.18 As a result, this treatment may be used not only to arrest enamel lesions but also to improve the esthetic appearance of buccal white spots.
As to <Case 1> and <Case 2>, the patients had history of orthodontic treatment and the white spot lesions were detected immediately after removal of fixed orthodontic appliances. To improve the remineralization, reinforcement of oral hygiene and fluoride varnish application was tried. However, the white spot still had existed for 10 years and 15 years. Therefore, change of treatment option is needed and decision was made to perform resin infiltration technique and microabrasion which are generally known as effective methods for correction of white spot lesions. As a result of microabrasion, white spot lesions look more whitish and opaque. On the other hand, significant size reduction of white spot lesion was detected in the resin infiltrated teeth.
Unfortunately, neither microabrasion nor resin infiltration technique can remove white spot lesions completely. The reason why some lesions are left after treatment could be thought that the depth of white spot lesion is not restricted to superficial part of enamel. It is reported that 200 µm of superficial enamel is removed by microabrasion and the depth of resin infiltration is about 60 µm.19 If the depth of white spot lesion is deeper than that of microabrasion or resin infiltration technique, it could still be detected. Therefore, caution should be taken for case selection.
In the limitation of this study, the findings of the present case report showed that resin infiltration technique seems to be more effective for correction of white spot lesion and caution should be taken for case selection.
- 1. Chang HS, Walsh LJ, Freer TJ. Enamel demineralization during orthodontic treatment. Aetiology and prevention. Aust Dent J. 1997;42(5):322-327.ArticlePubMed
- 2. Kang HS, Lee CY. The influence of the degree of saturation of acidulated buffer solutions in the root dentin demineralization. J Korean Acad Conserv Dent. 2004;29(5):454-461.Article
- 3. Sudjalim TR, Woods MG, Manton DJ. Prevention of white spot lesions in orthodontic practice: a contemporary review. Aust Dent J. 2006;51(4):284-289.ArticlePubMed
- 4. Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod. 1982;81(2):93-98.ArticlePubMed
- 5. Ogaard B, Rolla G, Arends J, ten Cate JM. Orthodontic appliances and enamel demineralization. Part 2. Prevention and treatment of lesions. Am J Orthod Dentofacial Orthop. 1988;94(2):123-128.ArticlePubMed
- 6. Cha SW, Yoon TC, Park SH, Lee CY, Kum KY. Quantitative analysis of mineral change in the initial carious lesion using confocal laser scanning microscopy. J Korean Acad Conserv Dent. 2001;26(1):1-8.
- 7. Kwun JW, Kim KY, Lee SJ, Jung IY, Lee CY. The effect of the supersaturated solutions containing high concentrations of fluoride on seeded crystal growth. J Korean Acad Conserv Dent. 1999;24(2):330-336.
- 8. Willmot DR. White lesions after orthodontic treatment: does low fluoride make a difference? J Orthod. 2004;31(3):235-242.ArticlePubMed
- 9. Al-Khateeb S, Extekate RA, de Josselin de Jong E, Angmar-Mansson B, ten Cate JM. Light-induced fluorescence studies on dehydration of incipient enamel lesions. Caries Res. 2002;36(1):25-30.ArticlePubMedPDF
- 10. Ardu S, Castiono NV, Benbachir N, Krejci I. Minimally invasive treatment of white spot enamel lesions. Quintessence Int. 2007;38(8):633-636.PubMed
- 11. Murphy TC, Willmote DR, Rodd HD. Management of postorthodontic demineralized white lesions with microabrasion: A quantitative assessment. Am J Orthod Dentofacial Orthop. 2007;131(1):27-33.ArticlePubMed
- 12. Donly KJ, O'neill M, Croll TP. Enamel microabrasion: a microscopic evaluation of the "abrosion effect". Quintessence Int. 1992;23(3):175-179.PubMed
- 13. Tong LS, Pang MK, Mok NY, King NM, Wei SH. The effects of etching, micro-abrasion, and bleaching on surface enamel. J Dent Res. 1993;72(1):67-71.ArticlePubMedPDF
- 14. Paris S, Meyer-Lueckel H, Kielbassa AM. Resin infiltration of natural caries lesions. J Dent Res. 2007;86(7):662-666.ArticlePubMedPDF
- 15. Robinson C, Hallsworth AS, Weatherell JA, Kunzel W. Arrest and control of carious lesions: a study based on preliminary experiments with resorcinol-formaldehyde resin. J Dent Res. 1976;55(5):812-818.ArticlePubMedPDF
- 16. Kielbassa AM, Gernhardt CR. Closing the gap between oral hygiene and minimally invasive dentistry: A review on the resin infiltration technique of incipient (proximal) enamel lesions. Quintessence Int. 2009;40(8):663-681.PubMed
- 17. Kidd EA, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83(Spec No C):C35-C38.ArticlePubMedPDF
- 18. Paris S, Meyer-Lueckel H. Masking of labial enamel white spot lesions by resin infiltration - A clinical report. Quintessence Int. 2009;40(9):713-718.PubMed
- 19. Davila JM, Buonocore MG, Greeley CB, Provenza DV. Adhesive penetration in human artificial and natural white spots. J Dent Res. 1975;54(5):999-1008.ArticlePubMedPDF
REFERENCES
Figure 1

<Case 1> Intraoral photographs taken prior to treatment (a), after completion of resin infiltration technique (right side) and microabrasion (left side) (b).
Figure 2

<Case 1> Photographs of left mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of microabrasion (b).
Figure 3

<Case 1> Photographs of right mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of resin infiltration technique (b).
Figure 4

<Case 2> Intraoral photographs taken prior to treatment (a) and after completion of resin infiltration technique (left maxillary central incisor), microabrasion (right maxillary central incisor) and resin composite restoration (right maxillary lateral incisor) (b).
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Clinical Effectiveness of Resin Infiltration and Fluoride Varnish for Managing White Spot Lesions (International Caries Detection and Assessment System (ICDAS) ≤ 2) During Multibracket Orthodontic Treatment: A Systematic Review and Meta-Analysis
Vilius Kosys, Gabija Streimikyte, Giedre Trakiniene
Cureus.2026;[Epub] CrossRef - Resin Infiltration for the Esthetic Improvement of Dental Fluorosis and White Spots: A Case Report
Sumayyah L Alkhudhayri, Shahad L Alhassani, Nada A AbdelAleem
Cureus.2024;[Epub] CrossRef - White spot lesions in fixed orthodontic treatment: Etiology, pathophysiology, diagnosis, treatment, and future research perspectives
Suma Shankarappa, Jerusha Titus Burk, Pradeep Subbaiah, Raghunath Nagasundara Rao, Vidya Gowdappa Doddawad
Journal of Orthodontic Science.2024;[Epub] CrossRef - White Spot Lesions in Fixed Orthodontics: A Literature Review on Etiology, Prevention, and Treatment
Deem Al-Blaihed, Omar El Meligy, Khlood Baghlaf, Rabab A Aljawi, Shahad Abudawood
Cureus.2024;[Epub] CrossRef - Effectiveness of low-viscosity resin infiltration (Icon) on color change of enamel white spot lesions: 1-year follow-up clinical study
Mohamed. H. Zaazou, Reham S. Saleh, Shahinaz N. Hassan, Ali Abdelnabi, Zeinab M. Zaki, Tamer M. Hamdy, Dalia Y. Zaki, Lamiaa M. Moharam
Bulletin of the National Research Centre.2024;[Epub] CrossRef - Individual tooth segmentation in human teeth images using pseudo edge-region obtained by deep neural networks
Seongeun Kim, Chang-Ock Lee
Signal Processing: Image Communication.2024; 120: 117076. CrossRef - Surface topography and spectrophotometric assessment of white spot lesions restored with nano-hydroxyapatite-containing universal adhesive resin: an in-vitro study
Neven S. Aref, Rahaf M. Alsdrani
BMC Oral Health.2023;[Epub] CrossRef - Infiltrating Resins, Noninvasive Treatment of White Spot Lesions: A Case Report
Rubén Darío Miranda-Carreño, Jacqueline Adelina Rodríguez-Chávez, Abigailt Flores-Ledesma
Journal of Oral Health and Community Dentistry.2023; 17(2): 75. CrossRef - Management of Turner's Hypoplasia Using Resin Infiltration: A Case Report
Dhruvi Solanki, Punit Fulzele, Nilima Thosar, Unnati Shirbhate
Cureus.2023;[Epub] CrossRef - Colour Parameters and Changes of Tea-Stained Resin Composite Exposed to Whitening Pen (In Vitro Study)
Abdulaziz Alhotan, Rasha M. Abdelraouf, Saleh Alhijji, Merry Angelyn Tan De Vera, Aref Sufyan, Jukka P. Matinlinna, Tamer M. Hamdy
Polymers.2023; 15(14): 3068. CrossRef - Effect of Resin Infiltration and Microabrasion on the Microhardness of the Artificial White Spot Lesions (An in Vitro Study)
Reem Majeed H.J. Al-Mamoori, Aseel Haidar M.J. Al Haidar
Journal of Baghdad College of Dentistry.2022; 34(1): 44. CrossRef - Effect of sodium fluoride plus tricalcium phosphate with and without CO2 laser on remineralization of white spot lesions
Nouran M. Eissa, Eman M. Elshourbagy, Nahla E. Gomaa
Heliyon.2022; 8(10): e10752. CrossRef - Efficacy of Resin Infiltration and Fluoride Casein Phosphopeptide Amorphous Calcium Phosphate Varnish on Non-cavitated Active White Spot Lesions in Children: A Randomized Clinical Trial
Mohit Dhamija, Rish Tyagi, Namita Kalra, Amit Khatri
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2022;[Epub] CrossRef - Individual Tooth Segmentation in Human Teeth Images Using Pseudo Edge-Region Obtained by Deep Neural Networks
Seongeun Kim, Chang-Ock Lee
SSRN Electronic Journal .2022;[Epub] CrossRef - In Vitro, Influence Of In-Office Dental Whitening On The Color Of Teeth Treated With Resin Infiltration
Basil Almutairi, Mohammed Al-Refai, Bander AL-Meshary, Abdulrahman Al-Asim, Fahad Al-Sharidah, Abdullah Alshehri
Annals of Dental Specialty.2021; 9(4): 6. CrossRef - Evaluation of color changes of white spot lesions treated with three different treatment approaches: an in-vitro study
Shaza M. Hammad, Noha A. El-Wassefy, Mohamed A. Alsayed
Dental Press Journal of Orthodontics.2020; 25(1): 26. CrossRef - Spectrophotometric Evaluation of Color Change in Tooth Enamel Defects Using Resin Infiltrate: An In Vivo Study
Anil Gupta, Shikha Dogra, Sakshi Joshi, Vimanyu Kataria, Jyotika Saini, Monika Nagpal, Payal Narula
International Journal of Clinical Pediatric Dentistry.2020; 13(2): 150. CrossRef - Erosion Infiltration in the Management of Molar‐Incisor Hypomineralization (MIH) Defects
Rym Mabrouk, Souha Yahia, Afef Oueslati, Nadia Frih, Yuk Kwan Chen
Case Reports in Dentistry.2020;[Epub] CrossRef - Pediatric Dentists’ Educational Experiences, Attitudes, and Professional Behavior Concerning Resin Infiltration: Implications for Dental Education
Michael Jordan Halcomb, Marita R. Inglehart, Elisabeta Karl
Journal of Dental Education.2020; 84(3): 290. CrossRef - Esthetic improvements of postorthodontic white-spot lesions treated with resin infiltration and microabrasion: A split-mouth, randomized clinical trial
Xi Gu, Lin Yang, Deqin Yang, Yuan Gao, Xiaolei Duan, Xin Zhu, He Yuan, Jiyao Li
The Angle Orthodontist.2019; 89(3): 372. CrossRef - Effect of resin infiltration on the color and microhardness of bleached white‐spot lesions in bovine enamel (an in vitro study)
Sidika Aynur Horuztepe, Meserret Baseren
Journal of Esthetic and Restorative Dentistry.2017; 29(5): 378. CrossRef - Effect of Resin Infiltration on Artificial Caries: Anin vitroEvaluation of Resin Penetration and Microhardness
Deepesh Prajapati, Rashmi Nayak, Deepika Pai, Nagraj Upadhya, Vipin K Bhaskar, Pujan Kamath
International Journal of Clinical Pediatric Dentistry.2017; 10(3): 250. CrossRef - Application of quantitative light-induced fluorescence to determine the depth of demineralization of dental fluorosis in enamel microabrasion: a case report
Tae-Young Park, Han-Sol Choi, Hee-Won Ku, Hyun-Su Kim, Yoo-Jin Lee, Jeong-Bum Min
Restorative Dentistry & Endodontics.2016; 41(3): 225. CrossRef - Non-destructive management of white spot lesions by using tooth jewelry
Hee-Jin Kim, Lorena Karanxha, Su-Jung Park
Restorative Dentistry & Endodontics.2012; 37(4): 236. CrossRef - Color and hardness changes in artificial white spot lesions after resin infiltration
Ji-Hoon Kim, Ho-Hyun Son, Juhea Chang
Restorative Dentistry & Endodontics.2012; 37(2): 90. CrossRef
 ePub Link
ePub Link Cite
CiteManagement of white spots: resin infiltration technique and microabrasion

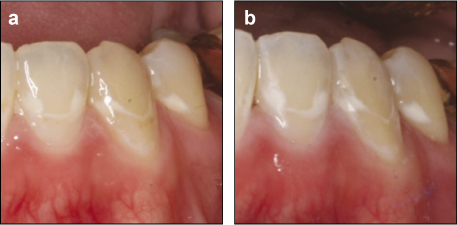
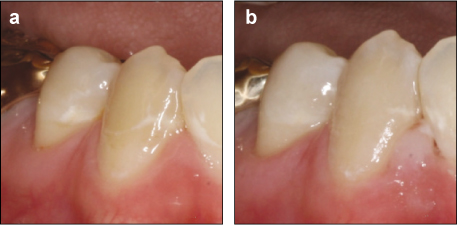
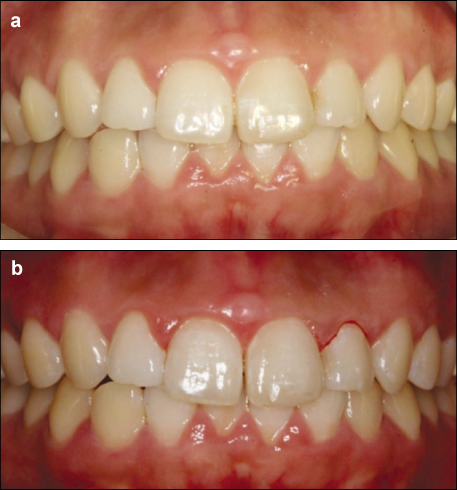
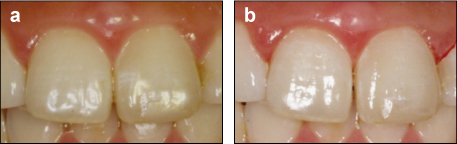
Figure 1
Intraoral photographs taken prior to treatment (a), after completion of resin infiltration technique (right side) and microabrasion (left side) (b).
Figure 2
Photographs of left mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of microabrasion (b).
Figure 3
Photographs of right mandibular lateral incisor, canine, second premolar taken prior to treatment (a), after completion of resin infiltration technique (b).
Figure 4
Intraoral photographs taken prior to treatment (a) and after completion of resin infiltration technique (left maxillary central incisor), microabrasion (right maxillary central incisor) and resin composite restoration (right maxillary lateral incisor) (b).
Figure 5
Photographs of maxillary central incisors taken prior to treatment (a) and completion of resin infiltration technique and microabrasion (b).
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Management of white spots: resin infiltration technique and microabrasion
Materials used
Table 1
Materials used

